Key Pharmacological Aspects of TPN Therapy and Drug Interactions
Understanding the Pharmacological Landscape of TPN Therapy
Total Parenteral Nutrition (TPN) is a critical intervention for patients with impaired gastrointestinal function, providing essential macro- and micronutrients through carefully formulated solutions. The pharmacological considerations surrounding TPN encompass compatibility, stability, drug-nutrient interactions, and safety protocols to optimize patient outcomes. This article explores these facets in depth, emphasizing the importance of coordinated multidisciplinary care, especially involving pharmacists, nurses, and clinicians.
Overview of TPN Components and Their Pharmacological Significance
What are the main components of TPN and their importance?
Total parenteral nutrition (TPN) is a comprehensive mixture designed to meet the nutritional needs of patients unable to feed orally or enterally. Its main components include macronutrients—lipids, proteins, and carbohydrates—and micronutrients such as vitamins, electrolytes, minerals, and trace elements.
Lipids typically account for 25-30% of total calories in TPN, providing essential fatty acids and aiding in energy density. Proteins, primarily amino acids, are essential for tissue repair, immune function, and metabolic processes, with adult requirements around 0.8-1 g/kg/day, though higher in critically ill patients. Carbohydrates are mainly delivered as dextrose, constituting 40-70% of total caloric intake, with a glucose utilization rate of about 5-7 mg/kg/min.
Micronutrients include vital vitamins—like A, C, D, E, K—and electrolytes such as sodium, potassium, calcium, magnesium, and phosphorus. Trace elements like zinc, copper, and selenium are also added in specific doses to support cellular functions and antioxidant defense.
How are adjustments made based on individual patient needs?
Clinicians should tailor TPN formulations to meet personal patient requirements. For example, protein doses vary according to clinical status—higher in trauma or burn patients and lower in renal failure. Electrolyte levels are also customized based on laboratory results and ongoing needs.
The lipid emulsions' composition can be adjusted for lipid tolerance, and carbohydrate delivery can be scaled according to blood glucose levels. Vitamins and trace elements are supplemented within safe ranges to avoid deficiencies or toxicities.
What implications do these components have for drug interactions?
The complex mixture in TPN can interact with various medications, affecting drug stability, efficacy, or safety. For instance, compatibility issues can arise with drugs like amiodarone and rifampin, which should not be coadministered via Y-site due to precipitation risks.
Lipids in TPN may impact drug pharmacodynamics by altering vitamin K activity or liver enzyme functions, potentially modifying drug metabolism. Moreover, adding drugs directly into the TPN bag is discouraged because of stability concerns and incompatibilities.
Pharmacists play an essential role in evaluating these interactions, ensuring safe combinations, and advising on separate administration routes when necessary. Proper monitoring and awareness of drug-nutrient interactions are critical to optimize patient outcomes and minimize adverse events.
| Component | Typical Content | Pharmacological Considerations |
|---|---|---|
| Lipids | 25-30% of calories; contains emulsifiers and triglycerides | Lipemia risk; interacts with certain drugs affecting stability |
| Proteins (Amino acids) | 0.8-1 g/kg/day, higher in critical illness | Affects drug metabolism; influences nitrogen balance |
| Carbohydrates (Dextrose) | 40-70% of calories; max utilization rate of 5-7 mg/kg/min | Risk of hyperglycemia; interacts with insulin management |
| Vitamins | ADEK, C, B-complex | Photosensitivity, oxidation; interactions affecting absorption |
| Electrolytes | Sodium, potassium, calcium, magnesium, phosphorus | Precipitation with calcium/phosphate; electrolyte imbalances affect drug action |
| Trace Elements | Zinc, copper, selenium | Insoluble salt formation; interference with drug stability |
Understanding these elements and their interactions helps optimize TPN therapy, ensuring nutritional adequacy while preventing adverse drug-nutrient interactions.
Nutritional Composition and Pharmacological Impacts
Main macronutrients and their percentages
Total parenteral nutrition (TPN) is a carefully formulated blend of essential nutrients designed to meet a patient's nutritional needs. It primarily includes lipids, proteins, and carbohydrates. Lipids typically provide about 25-30% of total caloric intake, serving as a dense energy source and supporting cell function. Proteins, made up of amino acids, fulfill critical roles in tissue repair and function, with adult requirements generally ranging from 0.8 to 1 gram per kilogram of body weight daily. This requirement increases in critically ill patients but decreases in those with renal failure. Carbohydrates are supplied mainly via dextrose, constituting about 40-70% of total calories, with a maximum glucose utilization rate of 5-7 mg per kg per minute to prevent hyperglycemia and metabolic disturbances.
Micro-Nutrients in TPN and Their Pharmacological Considerations
Vitamins, electrolytes, trace elements
Total Parenteral Nutrition (TPN) includes micro-nutrients such as vitamins, electrolytes, and trace elements to support metabolic functions and overall health. Vitamins like A, C, D, E, and K, along with trace elements such as copper, zinc, selenium, and chromium, are essential for various biochemical processes. Electrolytes including sodium, potassium, magnesium, calcium, and phosphorus help maintain fluid balance, nerve function, and muscle activity.
Daily recommended ranges
Each micro-nutrient in TPN must be carefully dosed within specific daily ranges to avoid deficiencies and toxicities. Sodium typically ranges from 135-145 mEq/L, magnesium from 8-20 mg/kg/day, calcium at 8-10 mg/kg/day, potassium from 40-60 mEq/L, and phosphorus around 15-20 mmol/day. Vitamins and trace elements have their own recommended daily doses, for example, vitamin C around 90-200 mg and zinc approximately 2.5-5 mg/kg/day, respectively. Precise adjustment tailored to the patient’s condition is crucial.
Potential interactions and instability risk
Micro-nutrients can interact with each other and with other components of TPN, influencing stability and safety. For instance, excessive calcium and phosphate levels can precipitate, risking catheter occlusion. Vitamin C can accelerate oxidation, and copper can catalyze the degradation of ascorbic acid. Light exposure, high temperature, and inappropriate pH can further degrade vitamins, while trace elements may form insoluble salts or destabilize lipid emulsions.
In practice, careful formulation and storage conditions, as well as monitoring blood levels, are necessary to ensure the safety and effectiveness of TPN. Understanding these pharmacological aspects of micro-nutrients helps prevent complications and optimizes nutritional outcomes for patients requiring parenteral nutrition.
Administration Routes and Compatibility Challenges
Central venous access options
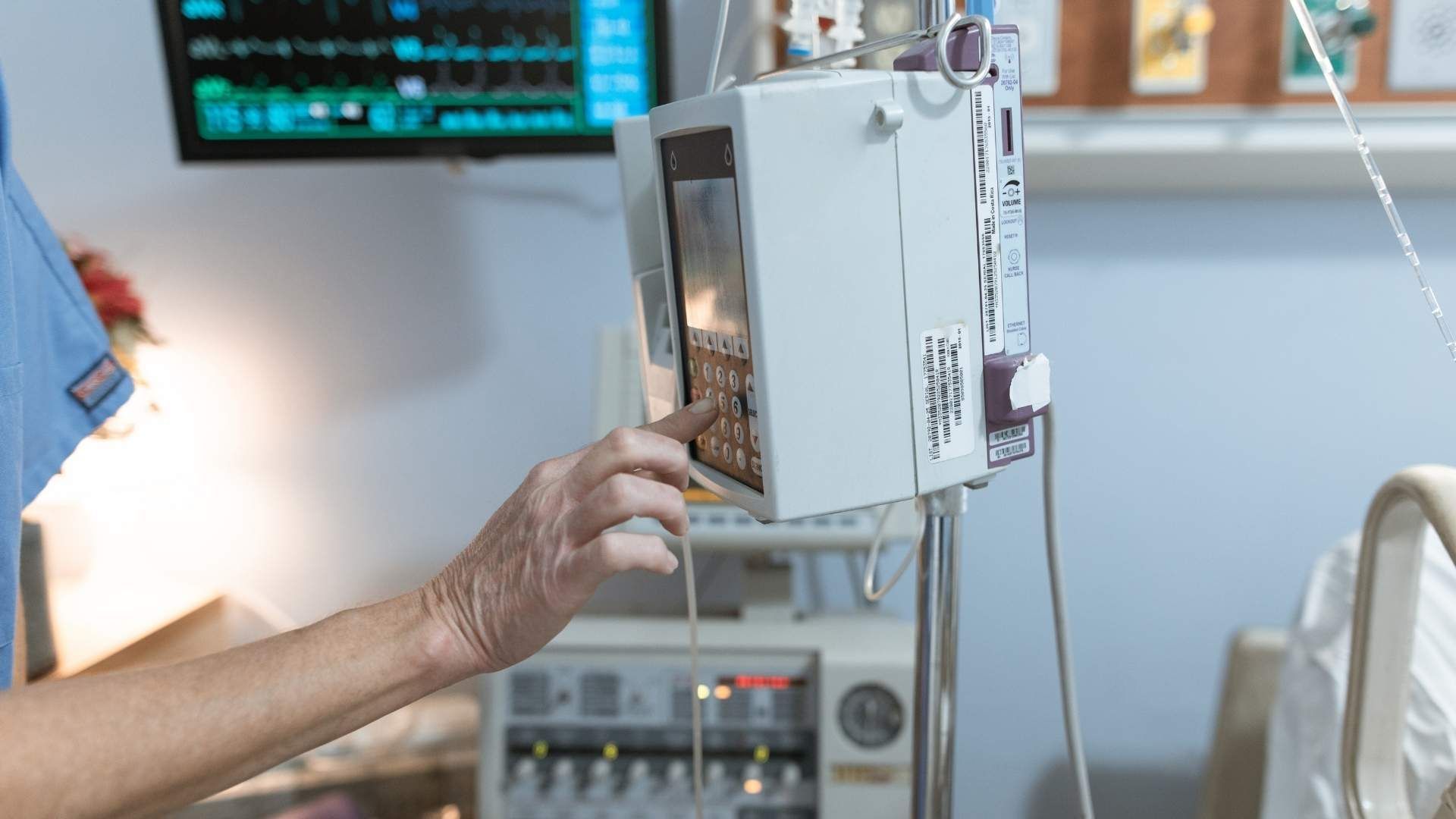
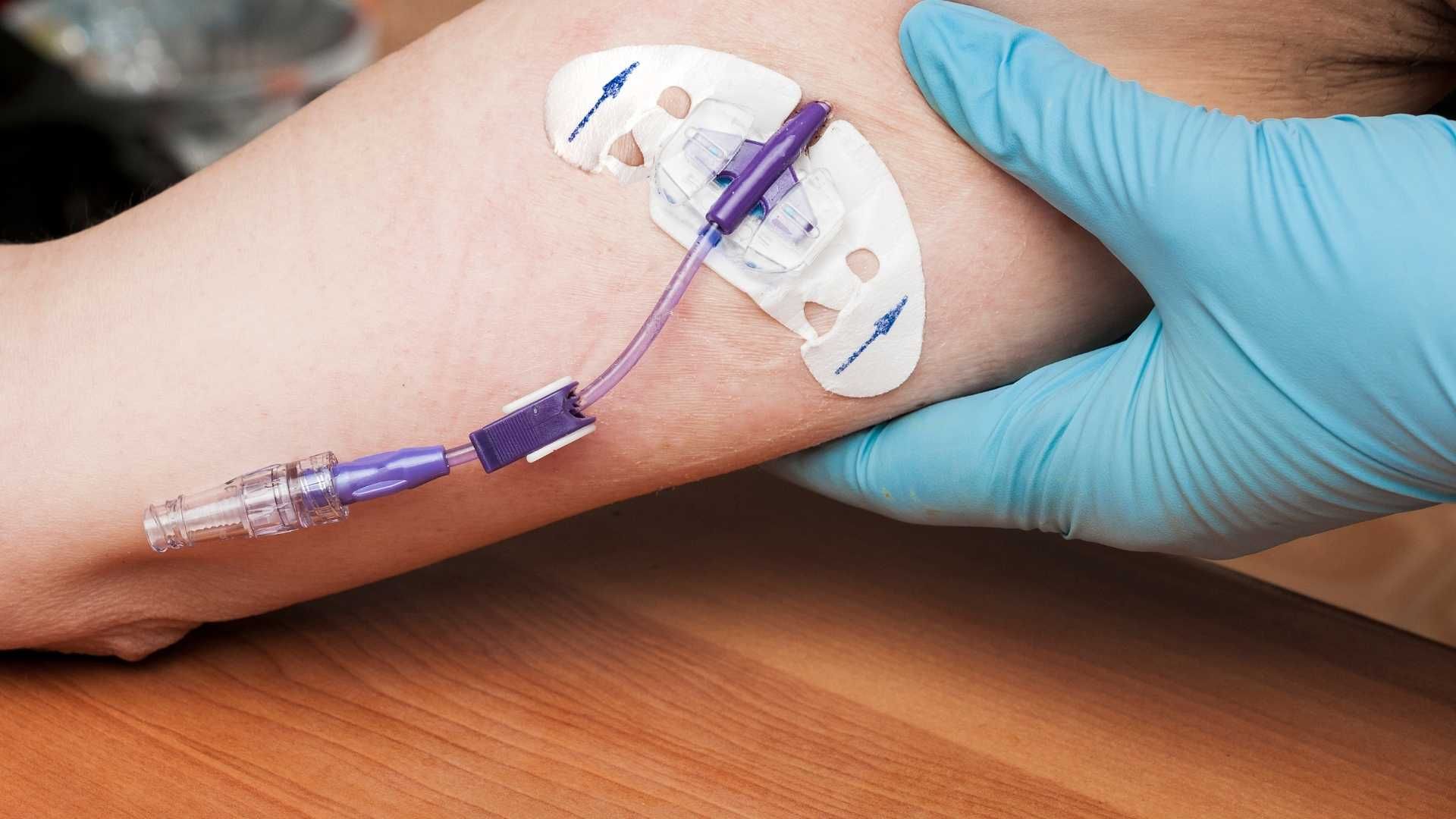
Total parenteral nutrition (TPN) requires insertion into a large vein, as its high osmolarity cannot be tolerated by peripheral veins. Common access points include peripherally inserted central catheters (PICC lines), central venous catheters (CVCs), and implantable ports. The choice depends on the duration of therapy, patient condition, and institutional protocols. These central devices allow delivery of nutrient mixtures directly into the bloodstream, ensuring rapid dilution and minimizing vein irritation.
Y-site compatibility and drug interactions
Administering drugs alongside TPN through Y-sites (where two infusion lines meet) demands careful consideration of drug compatibility. Some medications, such as amiodarone, phenobarbital, and rifampin, should not be co-infused with neonatal TPN due to risks like precipitation, which can have severe consequences such as embolism or catheter occlusion. Drugs need to be compatible in terms of pH, osmolarity, and chemical properties to prevent adverse reactions.
Risks of physical incompatibilities
Physical incompatibility refers to observable changes like precipitation, color shifts, or emulsion breakdown within the infusion line or container. These precipitates or destabilized emulsions can block catheters, reduce drug effectiveness, and cause complications such as phlebitis or emboli. For instance, combining calcium and phosphate in TPN solutions requires caution to prevent precipitate formation. Proper verification of compatibility, adherence to mixing protocols, and the use of separate lumens for medications and nutrition are vital strategies to mitigate these risks.
| Issue | Example | Potential Impact |
|---|---|---|
| Central access | PICC lines, CVCs, ports | Allows high osmolarity solutions to be safely administered |
| Y-site interactions | Amiodarone with TPN | Precipitation risk leading to embolism |
| Physical incompatibility | Calcium-phosphate precipitate | Catheter occlusion, embolism, reduced efficacy |
Ensuring optimal administration routes and compatibility involves collaboration among clinicians, pharmacists, and infusion specialists. Recognizing potential interactions and physical incompatibilities helps prevent complications and ensures safe, effective nutritional support.
Chemical and Physical Stability of TPN Components
Factors Influencing Stability
The stability of Total Parenteral Nutrition (TPN) components is critical to ensure patient safety and effective nutrition delivery. Several factors impact the chemical and physical stability of TPN formulations, including the composition of nutrients, environmental conditions, and storage practices. Compatibility between different ingredients such as amino acids, lipids, electrolytes, and vitamins must be carefully managed to prevent precipitation, emulsion breakdown, or oxidation, which can compromise sterility or efficacy.
Impact of pH, Light, Temperature
Environmental factors like pH, exposure to light, and temperature significantly influence TPN stability. For example, lipid emulsions are most stable around pH 8, and deviations from this pH can cause creaming or cracking of the emulsion. High temperatures accelerate chemical reactions leading to degradation of sensitive nutrients such as vitamins, especially vitamin C and vitamin A, which are highly susceptible to oxidation.
Light exposure can cause photodegradation of vitamins, reducing their potency over time. Similarly, oxygen exposure can promote oxidative reactions within the mixture, altering the stability of lipids and vitamins. Proper storage in opaque containers at controlled temperatures can mitigate these effects, prolonging the shelf life of TPN solutions.
Role of Amino Acids, Electrolytes, Vitamins
Amino acids act as both nutrients and stabilizers in TPN formulations; higher concentrations enhance emulsion stability by reducing calcium-phosphate precipitation risks. However, their acidity can sometimes lead to emulsion destabilization if not properly balanced. Electrolytes like calcium and phosphate need to be carefully combined, as their concentration ratios are critical to avoid precipitation of insoluble salts. Organic salts may improve compatibility, but overly concentrated electrolyte solutions can destabilize the mixture. Vitamins, especially water-soluble ones such as vitamin C and B-complex, are highly unstable and prone to degradation during preparation and storage. They must be added carefully, typically just before administration, and protected from light and heat.
Understanding and managing these factors are vital for maintaining the integrity of TPN formulations and ensuring safe, effective nutrition support. Collaboration among healthcare providers, including pharmacists and clinicians, is essential to optimize stability and prevent complications.
Compatibility and Incompatibility in TPN Formulations
Lipid Emulsions Stability
Lipid emulsions are crucial components of TPN, providing essential fatty acids and calories. Their stability depends on factors like pH, temperature, and the presence of stabilizing agents. Generally, the optimal pH for lipid emulsion stability is around 8. However, exposure to light, oxygen, or high temperatures can cause emulsion breakdown, leading to phase separation. Instability may manifest as creaming or cracking, reducing the effectiveness of the lipids and increasing the risk of embolism.
Calcium and Phosphate Interactions
Calcium and phosphate are vital minerals in TPN but are prone to forming insoluble precipitates when their concentrations and ratios are not carefully managed. Excessive calcium, combined with phosphate, can lead to precipitation, potentially occluding catheters or causing embolism. Using organic salts, such as calcium gluconate and potassium phosphate, can reduce this risk by enhancing component compatibility. Proper pH adjustment and controlling electrolyte concentrations are essential to prevent these incompatibilities.
Impact of High Osmolarity Solutions
High osmolarity solutions in TPN, like concentrated glucose or amino acids, are necessary for certain nutritional needs but can risk physical and chemical instabilities. These solutions increase the likelihood of precipitation with minerals and lipids, and can cause irritation if administered peripherally. Due to their osmolarity, TPN solutions are usually administered via central venous access, such as PICC lines or central catheters, to tolerate the osmotic load safely.
Compatibility Aspects Summary
| Component | Compatibility Concerns | Impact |
|---|---|---|
| Lipid emulsions | pH, temperature, oxygen exposure | Emulsion breakdown, phase separation |
| Calcium and phosphate | Concentration ratios, pH, salts | Precipitation, catheter occlusion |
| Osmolarity of solutions | Concentration of glucose, amino acids | Chemical instability, vascular irritation |
Understanding these factors helps prevent complications, ensuring the safe, effective, and stable delivery of total parenteral nutrition.
Drug Compatibility and Precautions for Co-Administration
What are the interactions with TPN?
Interactions between drugs and TPN components can significantly impact patient safety and therapeutic efficacy. These interactions can be categorized into several types, including physical incompatibilities, chemical reactions, and systemic effects.
Physical incompatibilities often manifest as precipitation, color changes, or emulsion breakdown. For example, certain drugs like amiodarone, phenobarbital, and rifampin should not be coadministered with neonatal TPN due to their potential to cause precipitates, which pose risks such as embolism or catheter occlusion.
Chemical incompatibilities involve reactions like lipid emulsion destabilization or precipitation of salts. Lipid emulsions are sensitive to pH and lipid content; adding incompatible drugs or solutions with high osmolarity can destabilize the emulsion, leading to embolic events.
Systemic interactions affect drug pharmacokinetics and pharmacodynamics. For instance, lipid emulsions in TPN can influence vitamin K levels and liver enzymes, potentially altering the metabolism of anticoagulants like warfarin, leading to resistance or increased bleeding risk.
Specific electrolyte interactions are also critical. Calcium and phosphate can form insoluble precipitates, especially when their concentrations are unbalanced. Organic salts and chelating agents may modify absorption or cause precipitation.
Adding drugs directly into TPN bags without proper compatibility assessment is generally discouraged. This practice can cause instability, precipitation, or microbial contamination, compromising safety.
Preferred administration methods
To minimize interaction risks, drugs should be administered through separate lumens or infusion lines whenever possible. For drugs with known compatibility issues, clinicians often recommend stopping TPN during the drug infusion or using intermittent administration techniques.
Timing is also essential. For drugs like phenytoin or fluoroquinolones, administering them either one hour before or two hours after TPN infusion can reduce negative interactions and improve absorption.
In some cases, specific drug formulations are preferred. For example, liquid preparations or IV formulations are recommended over crushed tablets, which might contain binders or coating that could precipitate or block the tube.
Monitoring plasma drug levels and patient response is crucial for drugs with narrow therapeutic indices. Pharmacists and healthcare providers should coordinate to adjust doses based on ongoing assessments.
In summary, careful consideration of drug compatibility with TPN, appropriate administration routes, and timing, combined with vigilant monitoring, can reduce risks associated with co-administration. This approach helps ensure both effective nutrition support and safe pharmacotherapy.
Pharmacological Effects of TPN on Drug Pharmacokinetics and Pharmacodynamics
How does TPN alter drug absorption, distribution, metabolism, and excretion?
Total parenteral nutrition (TPN) provides essential nutrients through a central vein but can also influence how medications behave within the body. These effects span across various pharmacokinetic processes, including absorption, distribution, metabolism, and excretion.
Firstly, TPN can directly impact drug absorption, especially when administered alongside enteral nutrition or through feeding tubes. Many drugs, such as phenytoin and levothyroxine, have reduced absorption when given with enteral feeds due to complexation with minerals or interaction with gastric pH changes. Additionally, the presence of nutrients can alter gastrointestinal motility and pH, further affecting drug dissolution and absorption.
In terms of distribution, lipids in TPN can influence how drugs bind to plasma proteins. For instance, lipid emulsions may alter the free (active) drug fraction, especially for highly lipophilic drugs. Changes in plasma volume and skin perfusion associated with nutritional status can also modify how drugs distribute throughout the body.
Metabolism is notably affected by TPN components, particularly lipids and vitamins that influence liver enzyme activity. For example, lipid emulsions can modify hepatic enzyme activity related to drug metabolism. Vitamins like vitamin K, supplied through TPN, can interfere with anticoagulant drugs such as warfarin, altering their expected effects.
Finally, TPN may influence drug excretion. Electrolyte imbalances caused by TPN, such as fluctuations in potassium or calcium, can alter renal function and subsequently affect how drugs are eliminated. Malnutrition or nutritional repletion can also modify renal or hepatic clearance processes, impacting drugs with narrow therapeutic windows.
Understanding these interactions is crucial for optimizing drug therapy in patients receiving TPN. Proper timing, dose adjustments, and monitoring are essential, especially for medications with significant pharmacokinetic considerations. Collaboration among healthcare providers, including pharmacists, is vital to ensure safe and effective medication management in these complex cases.
For more detailed insights, the impact of TPN on drug pharmacokinetics has been extensively reviewed, highlighting its influence on absorption, distribution, metabolism, and excretion processes.
Management of Blood Glucose and Metabolic Complications
What are the risks of hyperglycemia and hypoglycemia in TPN therapy?
Due to the high carbohydrate content of total parenteral nutrition (TPN), especially dextrose, there is a significant risk of developing blood sugar imbalances. Hyperglycemia, or elevated blood glucose levels, can occur when the body's insulin response is insufficient to handle the rapid influx of glucose. This condition can lead to dehydration, electrolyte imbalances, and increased susceptibility to infections.
Conversely, hypoglycemia, or low blood sugar, may develop if insulin doses are too high, or if TPN is halted abruptly without proper tapering. Both conditions can cause symptoms such as confusion, sweating, weakness, and in severe cases, coma.
How can monitoring strategies help in managing blood sugar levels?
Regular blood glucose monitoring is essential for patients receiving TPN, especially in critically ill or diabetic patients. Frequent checks—often every 4 to 6 hours—allow early detection of deviations from normal levels.
Monitoring methods include capillary blood glucose testing, which offers immediate feedback, and continuous glucose monitoring systems in some settings. Monitoring guides timely adjustments in insulin therapy or TPN composition to maintain blood glucose within a target range.
What is the role of insulin and blood sugar control in TPN?
Insulin plays a pivotal role in managing blood glucose levels in TPN patients. It can be administered via infusion or subcutaneously, depending on the patient's condition. Proper insulin dosing requires careful titration based on blood glucose measurements.
In some cases, adding insulin directly to the TPN bag is practiced, but it requires strict compatibility and stability considerations. Alternatively, insulin can be given through separate infusion lines or subcutaneously, which allows for better control.
Controlling blood sugar not only prevents acute complications but also reduces the risk of long-term issues such as infection, impaired wound healing, and cardiovascular problems. Overall, a multidisciplinary approach involving physicians, pharmacists, and nurses is crucial to optimize glycemic management during TPN therapy.
Drug-Nutrient Interactions and Their Clinical Significance
What are the mechanisms of interaction such as chelation, pH effects, and enzyme modulation?
Drug-nutrient interactions in TPN can occur through various mechanisms. Chelation is a common process where minerals like calcium and iron bind to certain drugs, forming insoluble complexes that reduce absorption and efficacy. For instance, calcium may precipitate when in contact with phosphate or certain antibiotics, leading to potential embolism if administered intravenously.
pH effects are also significant. Lipid emulsions in TPN are most stable at a pH around 8; deviations can cause creaming or cracking of emulsions, risking embolic events. Many drugs, like phenytoin, are pH-sensitive, and changes in the pH of the infusion solution or the GI tract can influence drug stability and absorption.
Enzyme modulation involves the influence of drugs and nutrients on metabolic enzymes such as CYP3A4. For example, grapefruit juice inhibits CYP3A4, increasing the bioavailability of certain medications like calcium channel blockers, which can lead to toxicity. Similarly, vitamin K levels in TPN impact warfarin effectiveness, demonstrating the systemic influence they can exert.
How do examples like warfarin, phenytoin, and vitamin K illustrate these interactions?
Warfarin's activity is affected by vitamin K content in TPN solutions. An increase in vitamin K can diminish warfarin's anticoagulant effect, risking clot formation, while decreased vitamin K can enhance bleeding risk. Adjusting the vitamin K levels in TPN or timing of warfarin administration is necessary.
Phenytoin absorption can be reduced when administered via enteral routes due to complexation with feeding components or altered transit time, demonstrating the importance of timing doses away from feeds. Crushing tablets and delaying administration are strategies to minimize interactions.
Vitamin K, essential for clotting, can be influenced by both systemic administration and dietary intake. Its balance is crucial when patients are on anticoagulants, and TPN formulations must be carefully managed to prevent interference with warfarin therapy.
What is the impact of these interactions on drug efficacy and nutrient absorption?
Interactions can significantly decrease drug efficacy; for example, calcium chelation can prevent antibiotics like tetracyclines from working effectively. Conversely, inhibition of enzymes such as CYP3A4 by grapefruit juice may increase drug levels, leading to toxicity.
Nutrient absorption is also compromised, seen with drugs like proton pump inhibitors reducing gastric acid and impairing vitamin B12 and iron absorption. These effects highlight the importance of coordinated medication and nutrition management.
Understanding these interactions allows clinicians and pharmacists to plan administration schedules, adjust doses, and select appropriate drug forms, ultimately improving patient safety and treatment outcomes.
Monitoring and Safety Strategies

Blood testing and infection control
Monitoring the patient’s blood parameters is essential for safe TPN administration. Regular blood tests help assess electrolyte levels, blood glucose, liver function, and nutritional status. Infections are a major concern with central venous access; strict aseptic techniques during insertion and maintenance of catheters are vital. Routine catheter site inspections and prompt removal of infected lines reduce the risk of bloodstream infections.
Liver function assessment
Long-term TPN use can impact liver health. Routine liver function tests (LFTs), including ALT, AST, alkaline phosphatase, and bilirubin, are used to detect early signs of liver dysfunction or cholestasis. Adjustments to the composition of TPN, such as reducing lipid infusion or modifying nutrient ratios, can mitigate liver damage. Continuous monitoring helps prevent progression to more severe hepatic conditions.
Electrolyte and glucose monitoring
Electrolytes like sodium, potassium, magnesium, calcium, and phosphorus should be checked frequently to prevent imbalances that can cause cardiac or neuromuscular issues. Blood glucose levels must be carefully managed, especially in diabetic patients or when high dextrose concentrations are used. Frequent glucose monitoring allows timely insulin adjustments or TPN modifications to maintain euglycemia.
Implementing a structured monitoring protocol ensures early detection of complications, allowing timely interventions. It involves collaboration among clinicians, pharmacists, and laboratory services to optimize safety and efficacy during TPN therapy.
Pharmacist's Role in TPN Optimization and Safety
What are the key pharmacological considerations for TPN?
Assessment of compatibility, stability, potential drug-nutrient interactions, and patient-specific adjustments are crucial.
Pharmacists play an integral role in ensuring the safe and effective use of TPN. They evaluate how different components and medications interact within complex nutritional formulations. This involves verifying the physical and chemical stability of TPN admixtures, and preventing incompatibilities such as precipitation or emulsion breakdown.
Preparation and compounding of formulations
Pharmacists are responsible for accurately preparing TPN solutions, ensuring correct concentrations and the proper order of mixing components. They must select appropriate additives and calculate doses tailored to each patient's needs. Proper sterile techniques and adherence to protocols are essential to prevent contamination and ensure safety.
Monitoring drug-nutrient interactions
Drug interactions within TPN can alter medication efficacy or cause adverse effects. For example, certain antibiotics or drugs like warfarin may have their activity affected by components such as lipid emulsions or vitamin K. Pharmacists should review all medications, monitor blood levels when required, and adjust dosing or administration schedules to mitigate these risks.
Incompatibilities such as precipitation of calcium salts with phosphate or destabilization of lipid emulsions due to drug interactions need vigilant oversight. Furthermore, drugs like phenytoin can bind to the feed components, reducing their absorption, so timing of administration is critical.
Patient education and multidisciplinary collaboration
Effective communication with healthcare teams and patients is vital. Pharmacists educate staff on proper administration techniques, potential interactions, and signs of TPN-related complications. They also collaborate with physicians, dietitians, and nurses to develop individualized nutrition plans, optimizing both nutritional status and medication therapy.
By integrating their specialized knowledge into the care team, pharmacists significantly contribute to improving patient safety, reducing complications, and enhancing overall outcomes during TPN therapy.
Emerging Research and Future Perspectives in TPN Pharmacology
Innovations in formulation stability
Recent advances in TPN formulation focus on enhancing the stability of nutrients and drugs to prevent degradation and incompatibility. Innovations include the development of new emulsifiers for lipid emulsions to improve stability at varying pH levels and temperature conditions. Enhanced electrolyte balancing strategies aim to minimize calcium-phosphate precipitations, which are common stability issues. Additionally, the incorporation of antioxidants and protective packaging helps prevent vitamin degradation due to light and oxygen exposure. These improvements aim to reduce complications and extend shelf life, ensuring safer and more reliable nutritional support.
Personalized nutrition approaches
Tailoring TPN regimens to individual patient needs has gained significant interest. Personalized approaches involve adjusting macronutrient ratios—such as lipids, proteins, and carbohydrates—to optimize metabolic responses and recovery. Incorporating genetic and metabolic profiling can predict nutrient utilization and drug responses, enabling precise adjustments. For critically ill or renal failure patients, fluid and electrolyte content can be customized for better outcomes. Advanced monitoring tools, including real-time blood glucose and electrolyte sensors, further support dynamic adjustments of TPN components, moving toward more effective and individualized nutritional therapy.
Advances in drug interaction mitigation
Efforts are underway to minimize adverse drug-nutrient interactions in TPN. Innovations include the development of compatibility charts and software that predict interactions based on formulation components. Additionally, new infusion techniques like multi-lumen catheters allow separate delivery of drugs and nutrition solutions, reducing physical interactions. Pharmacological research is also exploring drug formulations less susceptible to incompatibility—such as stable, lipophilic drug variants—and stabilizing agents that prevent precipitation or emulsion destabilization. These advances promise safer co-administration of medications and TPN, improving therapeutic efficacy and reducing risks.
| Aspect | Current Challenges | Future Directions |
|---|---|---|
| Formulation stability | Precipitation, oxidation, degradation | Advanced emulsifiers, antioxidants, protective packaging |
| Personalization | Variable patient needs, metabolic differences | Genetic data integration, real-time monitoring |
| Drug interaction mitigation | Compatibility issues, physical incompatibilities | Compatibility software, separate infusion sites, stable drug formulations |
As research progresses, the goal remains to enhance the safety, efficacy, and precision of TPN therapy, ultimately improving outcomes for diverse patient populations.
Summary and Key Takeaways
Critical elements of TPN pharmacology
Total parenteral nutrition (TPN) is a complex mixture of nutrients and additives tailored to meet individual needs. It mainly includes macronutrients such as lipids, proteins, and carbohydrates. Lipids account for 25-30% of total calories, proteins provide essential amino acids, and dextrose supplies energy, with most glucose used at a rate of 5-7 mg/kg/min. Micro-nutrients like electrolytes, vitamins, and trace elements are adjusted within recommended ranges to ensure safety and effectiveness.
TPN is usually administered through central veins, such as PICC lines or ports, due to its high osmolarity. Proper monitoring of blood glucose, triglycerides, and signs of liver or gallbladder issues is essential. Certain pharmaceuticals, like insulin and antibiotics, require careful compatibility checks to avoid precipitation or emulsion breakdown, which can lead to complications.
Management of interactions and stability issues
Drug and nutrient interactions in TPN can affect drug efficacy, absorption, and metabolism. For example, calcium and phosphate can precipitate, and some drugs like amiodarone or rifampin are incompatible with TPN solutions. Co-administration of drugs directly into TPN bags is generally discouraged unless stability data support it.
Stability of TPN components is influenced by factors such as pH, temperature, light, and oxygen exposure. Lipid emulsions are especially sensitive, requiring proper pH and emulsifier presence to remain stable. Trace elements like copper can accelerate vitamin degradation, and high osmolarity solutions can cause gastrointestinal issues.
Pharmacists play a pivotal role in ensuring stability and compatibility, adjusting formulations, and counseling healthcare teams on optimal practices to prevent precipitates, emulsion breakdown, or microbial proliferation.
Importance of multidisciplinary care
Managing TPN effectively involves a team approach, including physicians, pharmacists, dietitians, and nurses. Pharmacists' expertise in assessing drug-nutrient interactions, preparing compounded solutions, and monitoring therapy enhances patient safety.
Pharmacists also assist in planning drug administration routes, advising on timing to reduce interactions, and educating staff. Their involvement in quality control and monitoring is associated with improved outcomes, especially in complex or long-term TPN cases.
In conclusion, understanding the pharmacological nuances of TPN and fostering interdisciplinary collaboration is essential for safe, effective, and individualized nutritional support.
Concluding Remarks on Ensuring Safe and Pharmacologically Sound TPN Therapy
Optimizing TPN therapy requires a comprehensive understanding of its pharmacological intricacies, vigilant monitoring of potential drug interactions, and a collaborative approach among healthcare providers. Advances in formulation science, meticulous compatibility assessments, and proactive safety strategies are vital to prevent complications and improve patient outcomes. Pharmacists, nurses, and clinicians must work synergistically to tailor TPN therapy to individual patient needs, ensuring both efficacy and safety.
References
- Total Parenteral Nutrition - StatPearls
- Clinical nutrition and drug interactions - PMC
- Managing drug therapy in patients receiving enteral and ...
- Drug-Nutrient Considerations in Patients Receiving ...
- Parenteral Nutrition
- Drug/Nutrients Interaction in Neoplastic Patients Requiring Nutri
- Stability and compatibility of parenteral nutrition solutions
- Drug‐Nutrient Interactions - ASPEN Journals - Wiley
- Down the tube: Balancing enteral nutrition and medications