

Not all home infusion pharmacies are equal. Learn the 7 key questions to ask before choosing a specialty pharmacy, accreditation, clinical support, state licensing, and more.
Learn how home infusion therapy works for lupus (SLE), including Benlysta (belimumab) and other IV biologics, who qualifies for home treatment, and how Pharmko supports ongoing lupus care across 22+ states.

Learn how intraperitoneal nutrition (IPN) works for malnourished peritoneal dialysis patients, who qualifies, how amino acids are delivered during PD exchanges, and how Pharmko coordinates IPN therapy.

Pharmko is based in New York and provides home infusion therapy statewide — IV antibiotics, IVIG, TPN, IDPN, and specialty medications. Licensed, ACHC accredited, and available 24/7.

Osteomyelitis requires weeks of IV antibiotics that can often be completed at home. Learn who qualifies for OPAT, what the treatment timeline looks like, and how Pharmko supports bone infection recovery.
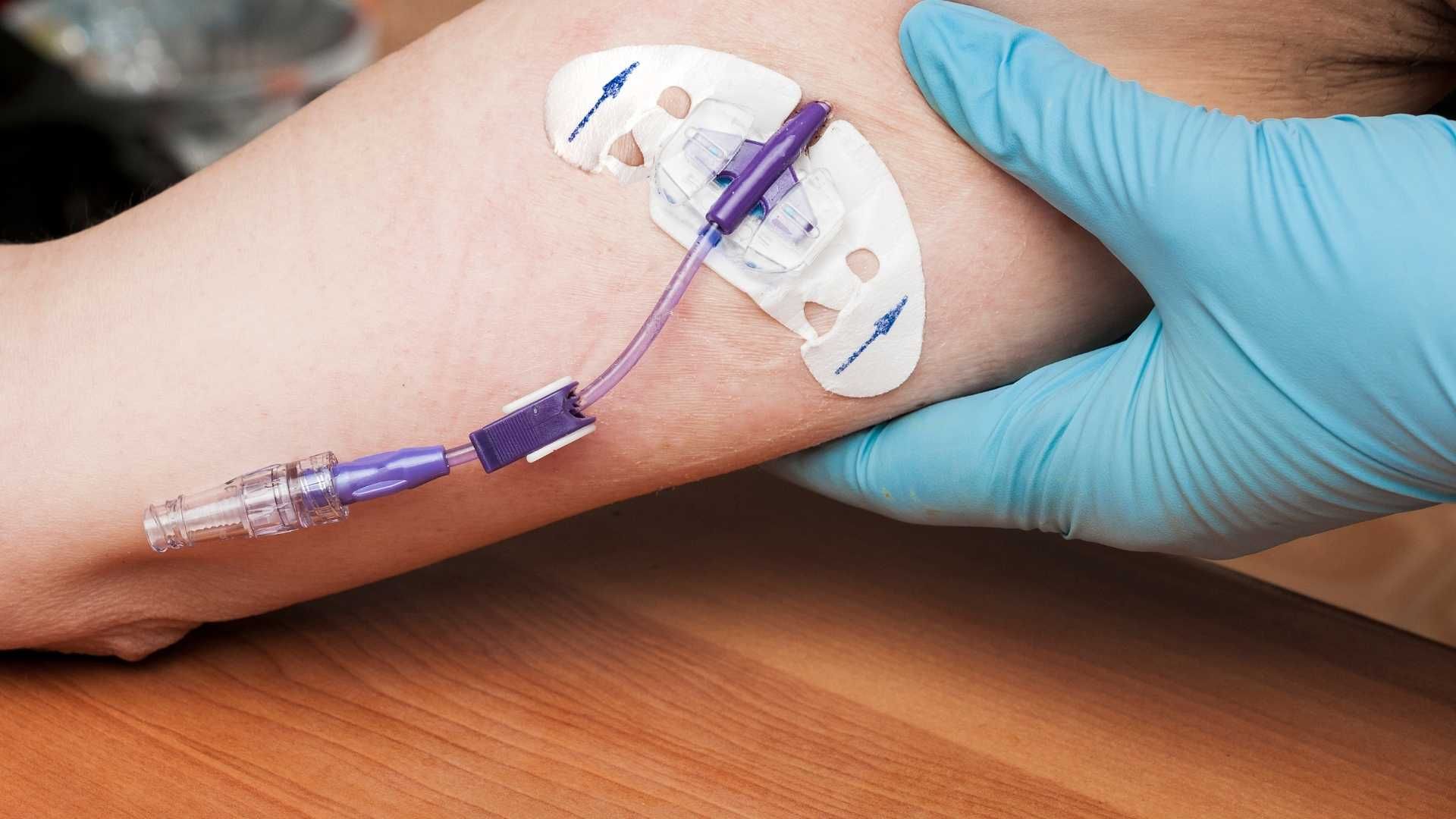
Learn what a PICC line is, how it's inserted, how to care for it at home, and why it's the most common IV access device for home infusion therapy. Pharmko nurses provide full PICC line training.

Learn how IV iron infusion works at home — which products are used, who qualifies, what to expect during treatment, and how Pharmko delivers iron infusion therapy across 22+ states.

Learn how home infusion therapy works for multiple sclerosis, including Ocrevus and Tysabri, who qualifies for home-based MS infusions, what to expect, and how Pharmko coordinates care.

Learn how total parenteral nutrition (TPN) at home works — who qualifies, how it's delivered, what daily life looks like, and how Pharmko supports patients from first dose through long-term therapy.

Low albumin is a key marker of malnutrition in dialysis patients. Learn what causes albumin decline, when IDPN is indicated, and how Pharmko supports renal nutrition across 22+ states.



