Understanding TPN-Associated Liver Disease
Exploring the Multifaceted Realm of TPN-Associated Liver Disease
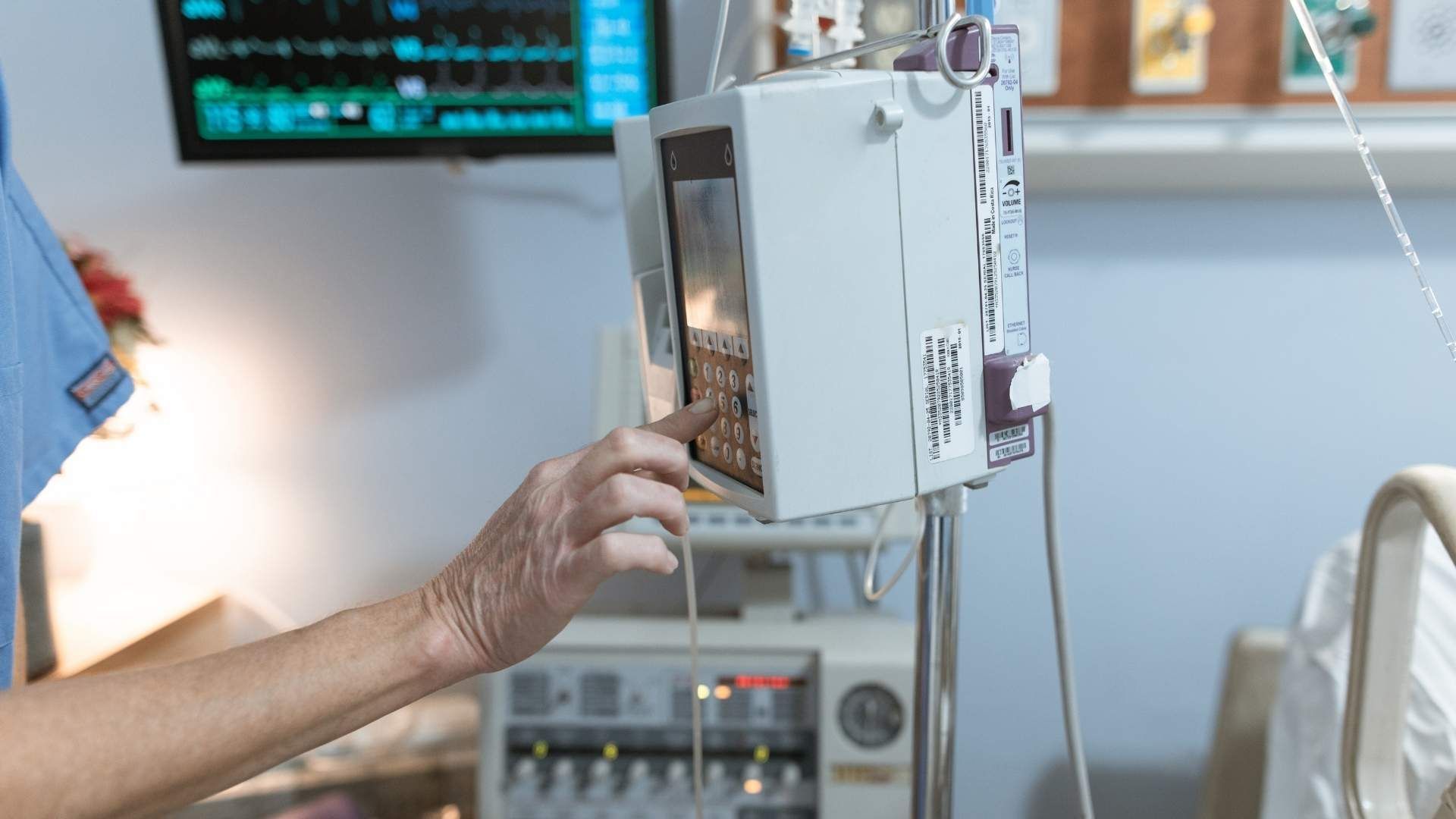
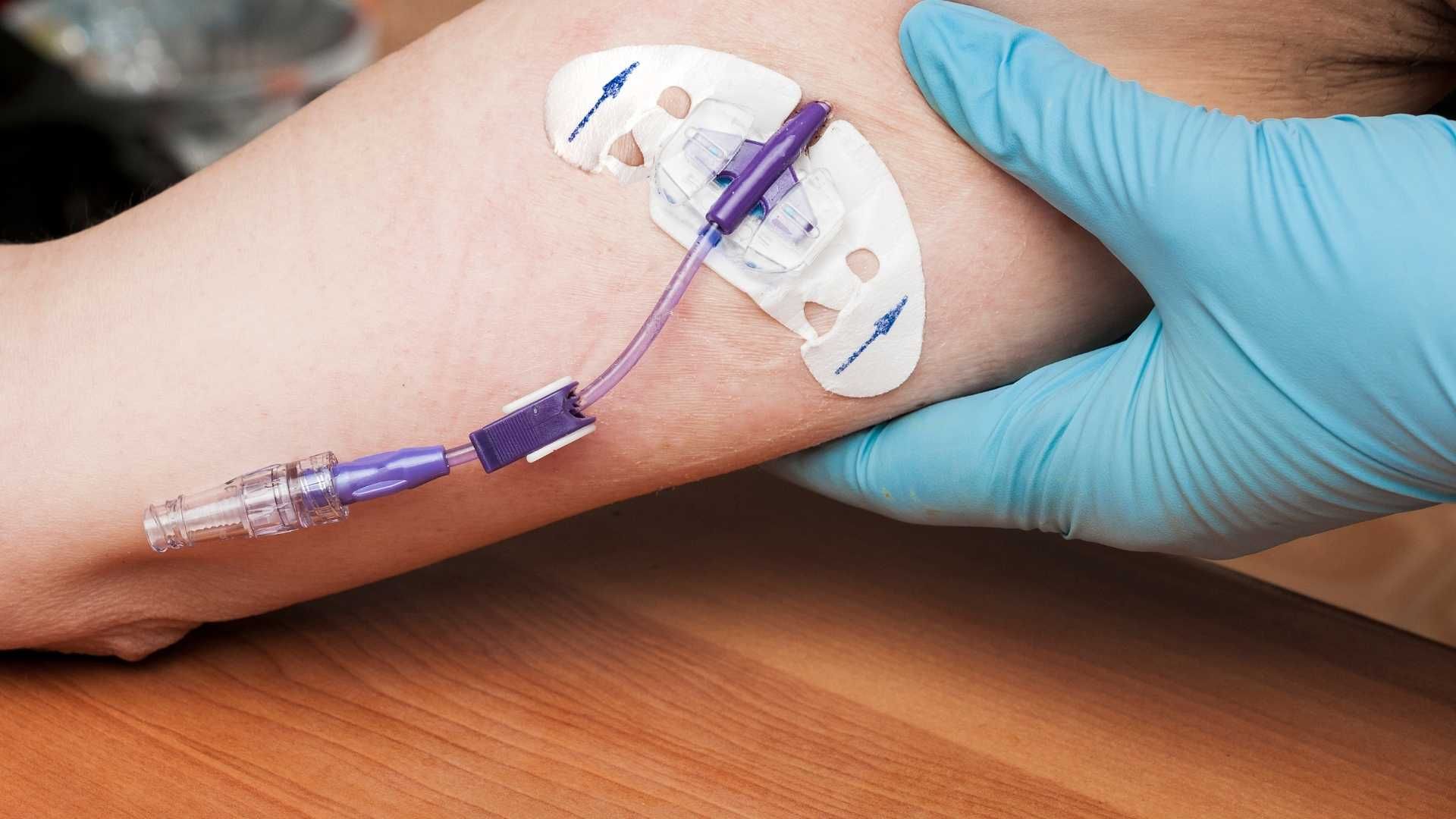
Total Parenteral Nutrition (TPN) has revolutionized care for patients with gastrointestinal failure and post-bowel surgery needs, yet its long-term application carries the significant risk of liver damage. Understanding the causes, mechanisms, clinical features, diagnostic criteria, management, and current research surrounding TPN-associated liver disease (PNALD) is crucial for optimizing patient outcomes and guiding future therapies.
Causes and Underlying Mechanisms of TPN-Associated Liver Disease
What are the causes and mechanisms of TPN-associated liver disease?
Parenteral Nutrition-Associated Liver Disease (PNALD) is a complex condition that develops due to numerous intertwined factors. Understanding these causes helps in managing and preventing the progressive liver damage observed in long-term TPN users.
One of the primary contributors is bacterial overgrowth within the gut, which results from impaired intestinal motility and lack of enteral stimulation. This overgrowth can lead to bacterial translocation, allowing endotoxins—particularly lipopolysaccharides—to enter the portal circulation. These endotoxins activate inflammatory pathways in the liver involving cytokines such as Tumor Necrosis Factor-alpha (TNF-α) and Interleukin-1 beta (IL-1β), which impair bile flow and promote hepatocyte injury.
Inflammation further exacerbates liver damage, often culminating in cholestasis—the impairment of bile secretion—leading to the accumulation of bile constituents within the liver and bloodstream. Recurrent infections, especially bloodstream infections related to catheters, amplify cytokine production and are recognized as significant risk factors.
In addition to infectious components, nutrient imbalances in TPN solutions contribute significantly. Excess caloric input, particularly from high glucose and lipid loads, causes hepatic steatosis—a buildup of fat within liver cells. Lipid overload, especially with soy-based emulsions containing phytosterols, intensifies this effect and has been associated with increased inflammation and cholestasis.
Nutrient deficiencies, notably of choline and taurine, also play crucial roles. Choline deficiency hampers phosphatidylcholine synthesis—necessary for lipid export from the liver—leading to fat accumulation and steatosis. This illustrates how both excesses and deficits in nutrients can disturb liver homeostasis.
Alterations in bile acid metabolism form another critical part of the pathogenesis. The gut microbiota, normally responsible for converting primary bile acids synthesized in the liver into secondary bile acids, becomes dysregulated in patients on TPN. Reduced enteral feeding and microbial imbalance lead to impaired bile acid transformation, further disrupting the enterohepatic circulation. An increase in gut microbial dysbiosis often favors bacteria like Proteobacteria, which can produce gases and toxins that damage intestinal and hepatic tissues.
The composition of lipid emulsions used in TPN is also pivotal. Soy-based lipid formulations rich in phytosterols are associated with increased liver inflammation and cholestasis, possibly due to their pro-inflammatory properties and interference with bile flow. Conversely, fish oil-based emulsions containing omega-3 fatty acids exhibit anti-inflammatory effects and are being investigated as therapeutic options to mitigate or reverse PNALD.
Chronic liver injury involves a cascade of events: hepatocyte injury, inflammation, fibrosis, and in severe cases, cirrhosis or liver failure. The constant activation of immune pathways and hepatic macrophages (Kupffer cells) perpetuates this cycle. Research continues to explore these pathways, with particular attention to cytokines like IL-1β, the NF-κB signaling pathway, and the Farnesoid X receptor (FXR), aiming for targeted treatments.
In summary, TPN-associated liver disease arises from an interplay of bacterial translocation, inflammatory cytokine activation impairing bile flow, nutrient-related damage, microbiota disruptions, and lipid emulsion composition. Managing these factors involves adjusting nutritional strategies, preventing infections, and exploring alternative lipid formulations to safeguard liver health in patients dependent on long-term TPN.
Clinical Presentation and Symptoms of TPN-Related Liver Damage
What are the common symptoms of TPN-associated cholestasis?
Patients receiving long-term TPN may exhibit a range of symptoms indicating liver dysfunction, particularly cholestasis. The most recognizable signs include jaundice, which manifests as a yellow discoloration of the skin and sclera (white part of the eyes). This occurs because of the accumulation of bilirubin when bile flow is impaired.
Dark urine is another prominent symptom, caused by increased conjugated bilirubin excreted through the kidneys. Conversely, pale or acholic stools are characteristic of bile flow obstruction, leading to a lack of bile pigments in the intestines.
Apart from direct signs of cholestasis, patients often report pruritus, which is an intense itching sensation resulting from bilirubin and bile salt deposition in the skin. Fatigue and general malaise are common as well, reflecting systemic effects of liver impairment.
More subtle symptoms may include poor feeding or appetite, weight loss, and abdominal discomfort or pain, particularly in the right upper quadrant where the liver is located. Swelling or edema can occur in severe cases due to hypoalbuminemia or portal hypertension. Nausea and vomiting may also be present, especially as liver damage progresses.
In pediatric populations, especially among infants, there might be a delay in symptoms, with some children remaining asymptomatic despite significant liver injury. These cases typically show abnormal liver function tests during routine assessments.
How does the progression of liver damage manifest clinically?
Over time, if the underlying issues such as nutrient imbalance or recurrent infections are not addressed, TPN-associated liver disease can advance from cholestasis to more severe states like fibrosis, cirrhosis, and ultimately liver failure. Signs of progression include worsening jaundice, increasing abdominal distension (due to ascites), easy bruising or bleeding, and signs of hepatic encephalopathy like confusion or altered mental status.
The clinical presentation varies depending on the severity and duration of liver injury, as well as individual patient factors including age and comorbidities. Prompt recognition of initial symptoms allows for early intervention, which can prevent or slow the progression to irreversible liver damage.
Diagnostic Strategies for TPN-Induced Liver Disease
How is TPN-associated liver disease diagnosed and detected?
Diagnosing parenteral nutrition-associated liver disease (PNALD) primarily revolves around a combination of biochemical assessments, imaging studies, and occasionally histological examination. The first step involves liver function tests, which typically reveal elevations in specific enzymes such as alanine aminotransferase (ALT), aspartate aminotransferase (AST), alkaline phosphatase (ALP), and gamma-glutamyl transpeptidase (GGT). Conjugated bilirubin levels are also measured, with elevations indicating cholestasis.
In most cases, biochemical changes emerge within 1 to 3 weeks after initiating TPN. Early biochemical markers, such as a 1.5-fold increase in GGT activity during the initial two weeks, can serve as predictors of developing liver disease.
Imaging techniques like ultrasound or computed tomography (CT) scans are valuable tools in supporting the diagnosis. They can visualize structural alterations in the liver, such as a coarse liver texture, capsular nodularity, the presence of ascites, and splenomegaly. These findings are indicative of ongoing liver pathology and can help differentiate PNALD from other hepatic conditions.
In instances where the diagnosis remains uncertain, or to evaluate the severity of liver damage, a liver biopsy might be performed. Although invasive and typically reserved for complicated cases, histological examination can reveal particular features like cholestasis, fatty infiltration (steatosis), fibrosis, and signs of inflammation.
A critical aspect of diagnosis involves ruling out other potential causas of liver impairment, including viral hepatitis, drug-induced liver injury, biliary obstructions, and metabolic liver diseases. Confirming the absence of these conditions helps in establishing a definitive diagnosis of PNALD.
| Diagnostic Method | Typical Findings | Additional Notes |
|---|---|---|
| Biochemical tests | Elevated ALT, AST, ALP, GGT; high bilirubin | Usually develops within 1-3 weeks of TPN; early markers useful |
| Imaging (ultrasound, CT) | Liver structural changes, splenomegaly | Supports biochemical findings; non-invasive options |
| Liver biopsy | Cholestasis, steatosis, fibrosis | Reserved for complex cases; provides detailed tissue info |
Management and Treatment Approaches for TPN-Related Liver Conditions
What are the management and treatment options for TPN-related liver conditions?
Managing liver disease caused by long-term parenteral nutrition (PN), such as PN-associated liver disease (PNALD), involves a multifaceted approach aimed at addressing underlying causes and improving liver function.
One of the primary strategies is optimizing the composition of TPN solutions. This includes reducing the lipid doses, ideally to less than or equal to 0.5 g/kg/day, to minimize lipid overload that contributes to fatty liver and cholestasis. Increasing Enteral Feeding is also crucial; early reintroduction of gut nutrition helps stimulate bile flow, maintain gut integrity, and reduce bacterial overgrowth.
Lipid modifications play a significant role in managing PNALD. Fish oil-based emulsions, such as Omegaven®, are rich in omega-3 fatty acids that have anti-inflammatory properties. These emulsions have been shown to reverse cholestasis and decrease liver inflammation. Replacing traditional soybean oil emulsions containing phytosterols—known hepatotoxic agents—can significantly improve liver outcomes.
Addressing infections and bacterial overgrowth is vital, as systemic infections and translocation of bacteria and endotoxins worsen liver injury. Treatments include antibiotics to control bacterial overgrowth and prevent sepsis, which exacerbates cholestasis through cytokine-mediated pathways.
Nutritional adjustments are also beneficial. Supplementation with nutrients like choline and taurine helps mitigate deficiencies that promote liver fat accumulation and cholestasis. Ensuring adequate mineral balance—limiting copper and manganese while maintaining zinc and selenium levels—can prevent additional hepatic burden.
Pharmacologic interventions, such as ursodeoxycholic acid, are used to improve bile flow and facilitate excretion of bile acids. These medications may provide symptomatic relief and slow disease progression.
In severe cases where liver damage progresses despite these measures, organ transplantation becomes necessary. Liver transplantation, sometimes combined with small bowel transplantation, offers definitive treatment for end-stage liver failure caused by PNALD.
Overall, managing TPN-related liver conditions relies heavily on early detection, adjusting nutritional support, and addressing secondary contributing factors to prevent progression to irreversible liver damage.
Preventive Strategies and Risk Factors for TPN-Associated Liver Problems
What are the risk factors and preventive measures for TPN-associated liver complications?
Parenteral nutrition-associated liver disease (PNALD) primarily affects patients who require long-term TPN, particularly infants and those with underlying gastrointestinal conditions. The development of liver complications is influenced by a combination of factors, with some being modifiable through strategic interventions.
Risk Factors
- Prolonged TPN Use: Extended duration of total parenteral nutrition increases the exposure time to potentially hepatotoxic components.
- Lack of Enteral Feeding: The absence of gut stimulation reduces the motility and secretion processes that help maintain normal bile flow.
- Overfeeding: Excess caloric intake, especially high doses of carbohydrates and lipids, can lead to fat accumulation in the liver, causing steatosis.
- Type of Lipid Emulsions: Soybean oil-based lipid emulsions rich in omega-6 fatty acids and phytosterols are linked to increased inflammation and impaired bile flow, contributing to PNALD.
- Infections and Sepsis: Bacterial translocation and bloodstream infections activate inflammatory cytokines such as TNF-α and IL-1β, further impairing liver function.
- Prematurity and Short Bowel Syndrome: These conditions predispose to alterations in gut microbiota, bacterial overgrowth, and nutrient deficiencies.
- Nutrient Deficiencies: Low levels of choline and taurine are associated with fatty liver development.
Preventive Measures
- Early Initiation of Enteral Feeding: Prompt introduction of enteral nutrition encourages gut motility, stimulates bile secretion, and helps maintain intestinal integrity.
- Monitoring and Adjusting Nutritional Content: Regular assessment of the TPN formulation allows for lowering carbohydrate and lipid delivery to safe levels—such as maintaining dextrose infusion rates ≤7 g/kg/day—to prevent overnutrition.
- Cycling Parenteral Nutrition: Alternating periods of infusion and fasting reduces continuous lipid and insulin exposure, decreasing hepatic fat accumulation and cholestasis risk.
- Selecting Appropriate Lipid Emulsions: Use of fish oil-based lipid emulsions like Omegaven® has demonstrated potential in reversing liver injury and reducing inflammation, owing to their omega-3 fatty acid content.
- Managing Infections and Bacterial Overgrowth: Vigilant infection control, prompt treatment of sepsis, and strategies to reduce bacterial translocation support liver health.
- Optimizing Gut Microbiota and Bile Flow: Strategies include avoiding unnecessary antibiotics and promoting physiological gut flora balance.
- Addressing Nutrient Deficiencies: Supplementing choline and taurine can mitigate fat accumulation and improve liver function.
By integrating these approaches, healthcare providers can significantly reduce the risk of developing TPN-related liver problems. The emphasis on careful nutritional management, infection control, and altering lipid formulations has shown to be effective in minimizing hepatic complications.
| Risk Factors | Preventive Measures | Additional Notes |
|---|---|---|
| Prolonged TPN use | Regular monitoring, early enteral feeding | Duration correlates with liver injury risk |
| Lack of enteral feeding | Initiate and advance enteral nutrition early | Maintains bile flow and gut integrity |
| Overfeeding (calories, carbs, lipids) | Adjust TPN composition, monitor infusion rates | Avoid caloric excess, keep dextrose ≤7 g/kg/day |
| Soy-based lipid emulsions | Use fish oil-based lipid emulsions | Rich in omega-3, reduces inflammation |
| Infections/sepsis | Infection prevention and timely treatment | Cytokine activation worsens liver injury |
| Prematurity and bowel length | Tailor nutrition, support gut maturation | Increase risk in infants with short bowel |
| Nutrient deficiencies (choline, taurine) | Supplement as needed | Mitigates hepatic steatosis |
This comprehensive approach can mitigate many risk factors, emphasizing the importance of individualized patient management and proactive nutritional strategies.
Types, Pathways, and Scientific Insights into Liver Damage caused by TPN
What are the different types and mechanisms of liver damage linked to TPN?
Parenteral nutrition (PN) can lead to a range of liver injuries, collectively known as PN-associated liver disease (PNALD) or intestinal failure-associated liver disease (IFALD). The primary forms of liver damage include cholestasis, steatosis, fibrosis, and cirrhosis.
Cholestasis is marked by impaired bile flow, resulting in elevated levels of alkaline phosphatase and conjugated bilirubin. It often manifests early during TPN therapy and can progress to liver fibrosis or failure if untreated. Steatosis, on the other hand, involves fat buildup within liver cells mainly due to excess caloric intake, especially high carbohydrate and lipid infusion, leading to fatty liver or steatosis. Over time, persistent steatosis can advance to fibrosis and cirrhosis.
The mechanisms underlying these injuries are complex and multifaceted. Lipid toxicity plays a crucial role, especially from soybean oil-based emulsions rich in omega-6 fatty acids, which are pro-inflammatory and impair bile flow. Excessive caloric intake promotes triglyceride accumulation, oxidative stress, and mitochondrial dysfunction. Bacterial translocation from the gut, particularly in patients with intestinal failure, triggers inflammatory pathways involving cytokines like tumor necrosis factor-alpha (TNF-α) and interleukins such as IL-1β, leading to cellular injury.
Nutrient deficiencies, notably of choline and taurine, can cause hepatic steatosis by disrupting lipid export and metabolism. Moreover, alterations in gut microbiota due to lack of enteral stimulation influence bile acid metabolism, further contributing to liver injury. Infections, especially sepsis and bacterial overgrowth, exacerbate damage through cytokine-mediated effects and endotoxin release.
Long-term use of TPN increases the risk of progressive liver damage, culminating in fibrosis and cirrhosis, especially when combined with other factors like nutrient imbalances and continuous infusion. Recognizing these pathways has driven research into preventative strategies, including optimizing TPN formulations, promoting early enteral feeding, and utilizing lipid emulsions containing omega-3 fatty acids.
How do lipid components like phytosterols and omega-3 fatty acids influence liver health?
Lipid components of TPN are central to the development or prevention of liver damage. Traditional soybean oil-based emulsions contain phytosterols, plant-derived compounds that are believed to inhibit bile flow and promote inflammation, thereby contributing to cholestasis and steatosis.
Recent advances have introduced fish oil-based lipid emulsions, rich in omega-3 polyunsaturated fatty acids (PUFAs), which are anti-inflammatory and have been shown to improve liver histology in cases of PNALD. These emulsions, such as Omegaven®, reduce pro-inflammatory mediators and promote resolution of hepatocellular injury.
In contrast, omega-6 fatty acids prevalent in classic soybean emulsions tend to promote inflammatory cascades. The balance between omega-3 and omega-6 fatty acids in lipid emulsions influences inflammatory responses and liver outcomes.
What is the progression from initial liver injury to fibrosis and cirrhosis?
Persistent liver injury from long-term TPN use can lead to progressive scarring. Initially, fat accumulation and cholestasis may be reversible with adjustments in therapy and nutritional support.
However, ongoing inflammation, bacterial translocation, and cellular injury activate hepatic stellate cells and promote extracellular matrix deposition, leading to fibrosis. Over time, sustained fibrosis can evolve into cirrhosis, impairing liver function and increasing the risk of liver failure.
How do molecular pathways involving cytokines, hepatic macrophages, and transporters play a role?
Research into the molecular basis of PNALD has highlighted the roles of cytokines such as IL-1β and TNF-α, which mediate inflammatory responses. Activated hepatic macrophages (Kupffer cells) respond to bacterial products and phytosterols, releasing cytokines that further impair bile transporter activity.
Pathways involving nuclear factor-kappa B (NF-κB) and Farnesoid X receptor (FXR) are also under investigation. These pathways regulate inflammation and bile acid homeostasis, respectively.
Understanding these complex interactions has led to hypotheses about targeted therapies that could modulate inflammatory responses or enhance transporter function, offering hope for preventing or reversing severe liver damage in patients on long-term TPN.
| Aspect | Details | Additional Notes |
|---|---|---|
| Liver injury types | Steatosis, cholestasis, fibrosis, cirrhosis | Occur sequentially or overlap in time |
| Main mechanisms | Lipid toxicity, inflammation, bacterial translocation, nutrient deficiency | Multifactorial process |
| Lipid components | Soy-based (pro-inflammatory, phytosterols); Fish oil-based (anti-inflammatory) | Impact depends on composition |
| Progression path | Steatosis → Fibrosis → Cirrhosis | Long-term injury increases severity |
| Molecular pathways | Cytokines, macrophages, transporters (BSEP, NTCP) | Targets for potential therapies |
Understanding the diverse pathways and factors involved in TPN-related liver damage helps guide clinicians in preventing progression and tailoring therapeutic approaches to maintain liver health in patients dependent on long-term parenteral nutrition.
Ongoing Research, Molecular Pathways, and Future Perspectives in TPN-Related Liver Disease
What is the current scientific understanding and ongoing research regarding TPN-associated liver disease?
Parenteral nutrition-associated liver disease (PNALD) is recognized as a common complication in patients receiving long-term total parenteral nutrition (TPN). It is a result of complex interactions involving disrupted bile acid metabolism, bacterial translocation, and nutrient toxicity. The pathogenesis is multifactorial, involving inflammation, oxidative stress, endoplasmic reticulum (ER) stress, and mitochondrial dysfunction.
Recent advances in science have provided deeper insights into these mechanisms. For instance, studies utilizing transcriptomics and metabolomics have revealed significant alterations in lipid, cholesterol, and energy pathways within the liver, indicating a disturbed metabolic environment. These technologies enable researchers to identify specific biomarkers associated with disease progression, facilitating earlier diagnosis and targeted intervention.
A key area of research focuses on optimizing nutritional formulations. Various lipid emulsions, especially those enriched with omega-3 fatty acids from fish oil, are under investigation for their ability to reduce inflammation and improve liver function. Additionally, strategies to minimize infection rates—such as rigorous infection control and early enteral nutrition—are crucial in the prevention of PNALD.
Despite this progress, many molecular details remain unclear. Researchers are exploring the exact cellular and genetic triggers that initiate liver injury, with a particular focus on vulnerable groups like infants. The goal is to identify reliable biomarkers for early detection and to develop pharmacological interventions that can halt or reverse disease progression.
The future of PNALD management lies in precision medicine—tailoring nutritional and pharmacological approaches based on individual patient profiles. This entails a multidisciplinary effort combining advanced molecular research, clinical trials, and innovative therapeutic development.
In summary, ongoing research aims to unravel the complex molecular pathways involved in PNALD, with a strong emphasis on understanding the roles of inflammation and gut microbiota, and on developing targeted treatments. These efforts are paving the way for more effective prevention, early diagnosis, and personalized therapy strategies, promising better outcomes for patients dependent on long-term TPN.
Looking Forward: Improving Outcomes and Unraveling Complex Pathways
Advances in understanding the multifaceted mechanisms of TPN-associated liver disease have opened new avenues for prevention, early diagnosis, and targeted treatment. Continued research into molecular pathways, innovative lipid formulations, and optimal nutritional strategies holds promise for reducing the burden of liver complications in patients dependent on parenteral nutrition. A multidisciplinary approach, combining clinical vigilance with cutting-edge scientific insights, is essential to improve long-term liver health and overall quality of life for these vulnerable patients.
References
- Review of parenteral nutrition-associated liver disease - PMC
- TPN and Liver Damage: A Comprehensive Overview
- Parenteral Nutrition–Associated Liver Disease - PMC
- Understanding Intestinal Failure-Associated Liver Disease
- Understanding TPN-Related Transaminitis: Causes & ...
- Parenteral nutrition-associated liver disease and lipid ...
- Pathogenesis and treatment of parenteral nutrition- ...
- Management of PN-induced Cholestasis
- Treatment of Parenteral Nutrition-Associated Liver Disease
- Pathogenesis and treatment of parenteral nutrition- ...