Understanding TPN’s Role in Managing Sepsis and Septic Shock
Exploring the Nuances of Nutritional Support in Septic Care
Sepsis and septic shock are complex syndromes requiring rapid, tailored interventions to improve survival and long-term recovery. Nutritional support, particularly the use of Total Parenteral Nutrition (TPN), plays a controversial yet significant role within this context. This article examines the physiological rationale, clinical implications, and current debates surrounding TPN in the management of sepsis and septic shock, emphasizing evidence-based practices and emerging research.
The Pathophysiology of Sepsis and Its Impact on the Gut
What is the significance of systemic inflammation in sepsis?
Sepsis triggers an uncontrolled inflammatory response throughout the body, characterized by the release of cytokines such as TNF, IL-1β, and IFN-γ. These mediators promote widespread tissue damage, endothelial activation, and increased vascular permeability. The inflammatory cascade can result in systemic organ dysfunction, affecting the lungs, kidneys, liver, and cardiovascular system.
How does gut barrier dysfunction contribute to sepsis progression?
The gastrointestinal (GI) tract plays a pivotal role in sepsis development due to its unique immune environment and abundant microbiota. During sepsis, inflammation compromises the intestinal mucosal barrier, leading to increased permeability, ulceration, and damage. This breach allows translocation of bacteria and endotoxins from the gut lumen into the bloodstream, fueling systemic infection and inflammation.
What role does microvascular thrombosis play in organ hypoperfusion?
Sepsis induces coagulation activation, resulting in microvascular thrombosis. These tiny clots obstruct blood flow at the capillary level, impairing tissue perfusion and oxygen delivery. The subsequent organ hypoperfusion exacerbates tissue ischemia, promotes further cellular injury, and propagates a vicious cycle of worsening organ dysfunction.
How does organ hypoperfusion relate to sepsis severity?
Persistent hypoperfusion is a hallmark of septic shock, characterized by inadequate blood flow to vital organs despite resuscitation efforts. This state leads to multiple organ failure, including acute respiratory distress syndrome (ARDS), acute kidney injury, and hepatic dysfunction. Restoring adequate perfusion through fluid resuscitation and vasopressors is fundamental in sepsis management.
| Aspect | Impact | Mechanism/Example |
|---|---|---|
| Systemic inflammation | Widespread organ damage | Cytokine storm damages tissues and endothelium |
| Gut barrier dysfunction | Increased infection risk | Mucosal damage allows bacteria translocation |
| Microvascular thrombosis | Organ hypoperfusion | Capillary microthrombi block blood flow |
| Organ hypoperfusion | Organ failure | Reduced perfusion causes cell death and tissue injury |
Effective strategies for managing sepsis and septic shock
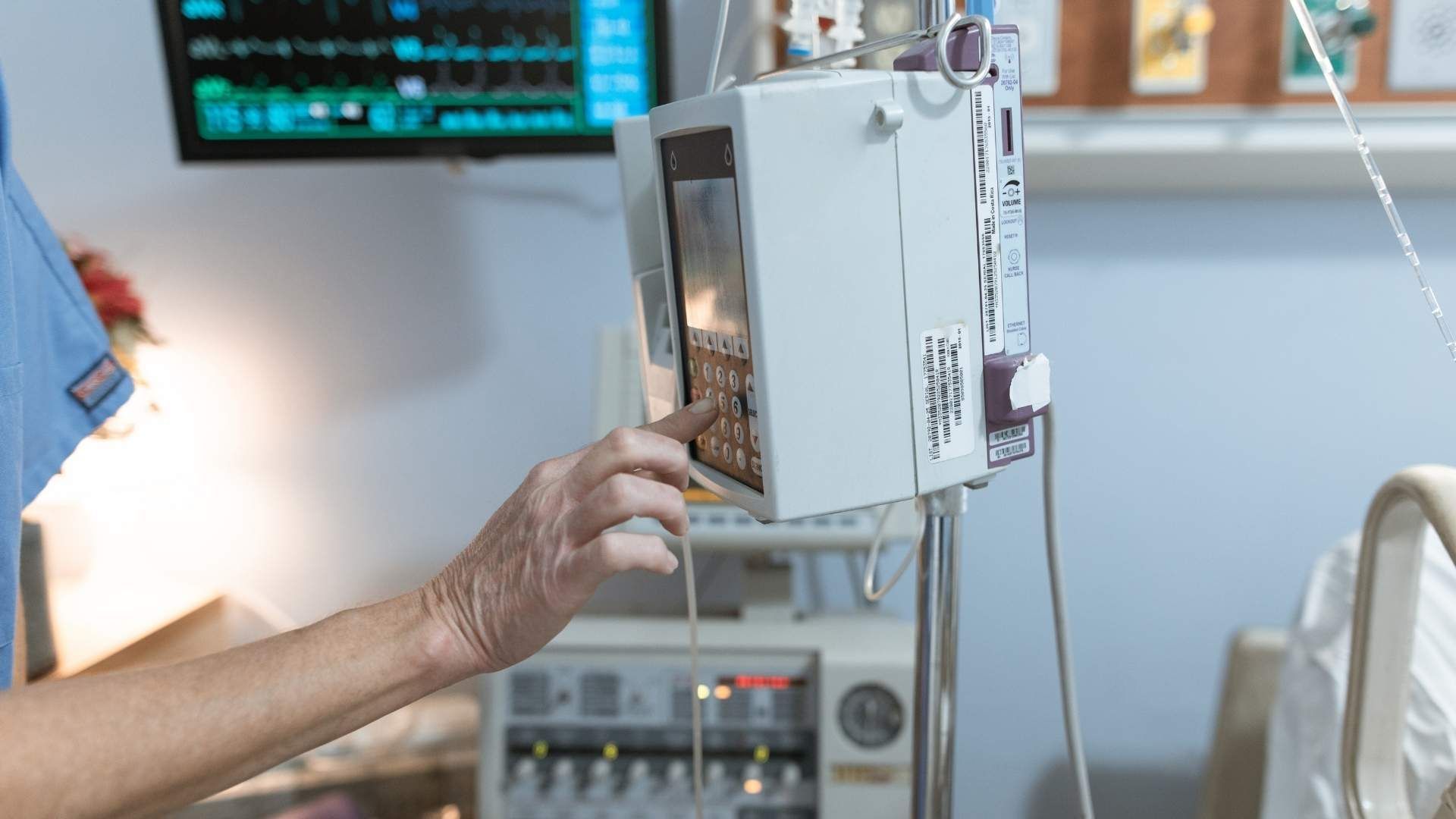
The cornerstone of sepsis management lies in early recognition and prompt treatment. First-line strategies include administering broad-spectrum antibiotics swiftly to target pathogens and initiating aggressive IV fluid resuscitation to stabilize blood pressure. Vasopressors, such as norepinephrine, are employed if fluid resuscitation alone cannot maintain adequate perfusion. Continuous monitoring of vital signs, lactate levels, and organ function guides treatment adjustments.
Source control is essential, involving diagnostics and, when necessary, surgical intervention to remove infection sources. Supportive measures like oxygen therapy, mechanically assisted ventilation, and renal replacement therapies are implemented depending on the individual patient's needs.
Nutritional support also plays a crucial role. As sepsis induces a hypermetabolic state, tailored nutritional interventions—preferably enteral nutrition—help preserve immune function, reduce infection risks, and promote tissue repair. Balancing caloric and protein intake is vital to prevent complications. When enteral feeding fails or is contraindicated, parenteral nutrition may be used cautiously, considering its risks.
| Treatment Aspect | Approach | Rationale |
|---|---|---|
| Antibiotics | Early broad-spectrum administration | Target infection, prevent progression |
| Fluid resuscitation | IV fluids, vasopressors if needed | Maintain perfusion and blood pressure |
| Organ support | Ventilation, dialysis, supportive care | address organ failures, prevent deterioration |
| Nutritional support | Enteral preferred; TPN if necessary | Support metabolic demands and immune function |
The importance of nutrition assessment and management
Nutrition significantly influences sepsis outcomes. Pre-illness malnutrition predisposes patients to worse courses. Screening for nutritional risk early in sepsis diagnosis helps guide intervention.
Early enteral nutrition may help maintain gut integrity and immune defenses, reducing bacterial translocation and secondary infections. It is recommended to provide about 1.0 g/kg/day of protein and moderate calories (~15 kcal/kg/day) during the initial phase, emphasizing micronutrients and vitamins.
Post-resuscitation, increased protein intake (1.5–2.0 g/kg/day) and caloric support facilitate recovery and lean body mass restoration. Long-term nutritional strategies, including high-protein oral supplements, are necessary for months to years after ICU stay to improve functional outcomes.
| Nutrition Strategy | Timing and Components | Expected Benefit |
|---|---|---|
| Pre-illness assessment | Screening for malnutrition and risk | Tailors interventions, prevents deterioration |
| Early enteral nutrition | Initiate within 24-48 hours if feasible | Maintains gut barrier, reduces infections |
| Post-resuscitation | Increased protein (1.5-2.0 g/kg/day) | Promotes muscle mass, supports recovery |
| Long-term nutrition | High-protein supplements for months/years | Supports functional and physical recovery |
Why TPN is contraindicated in sepsis
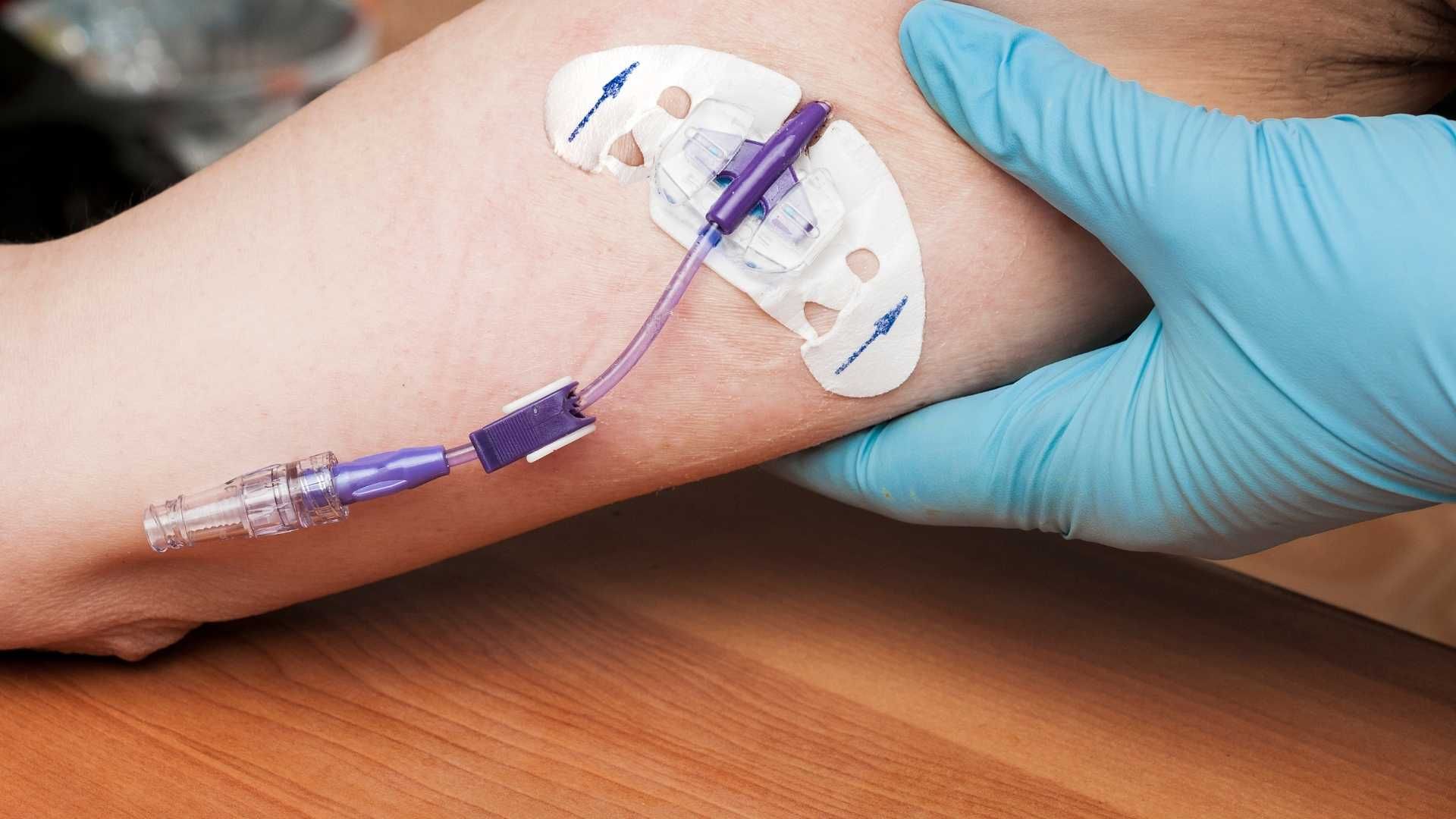
Total parenteral nutrition (TPN) is generally avoided in septic patients because it may worsen outcomes. Evidence suggests TPN can promote bacterial growth, including resistant strains, by providing an abundant source of nutrients directly into the bloodstream.
Furthermore, TPN use in sepsis is associated with an increased risk of bloodstream infections due to central line usage, immune suppression, and metabolic disturbances such as hyperglycemia. It can also impair gut mucosal integrity, reducing the beneficial effects of enteral nutrition.
The study highlights that TPN's potential to exacerbate infection and immune suppression outweighs its benefits during active sepsis. When enteral nutrition is not tolerated, cautious use of TPN may be considered, but only after evaluating the overall risk-benefit ratio and under strict infection control protocols.
| TPN Risks in Sepsis | Implication | Why It Is Usually Avoided |
|---|---|---|
| Increased infection risk | Bloodstream infections from central lines | Promotes bacterial translocation and resistant strains |
| Immune suppression | Reduced immune response | Can worsen infection severity |
| Metabolic disturbances | Hyperglycemia, liver dysfunction | Exacerbates illness, impairs recovery |
By understanding these complex mechanisms and strategies, clinicians can optimize sepsis management, emphasizing early, targeted, and individualized approaches that include the appropriate use of nutritional support.
The Evidence Against Routine Use of TPN in Sepsis
What are the most effective management strategies for sepsis and septic shock?
Managing sepsis and septic shock effectively hinges on swift recognition and prompt initiation of targeted treatment. The cornerstone strategies include early broad-spectrum antibiotics to combat the infection, combined with aggressive intravenous fluid resuscitation aimed at maintaining adequate blood pressure and ensuring vital organ perfusion. Vasopressors, such as norepinephrine, are often employed if fluid therapy alone fails to stabilize hemodynamics.
Supportive interventions like oxygen therapy, mechanical ventilation, and dialysis help maintain organ function. Identifying the infection source via diagnostics and surgical intervention is critical for definitive treatment. Continuous assessment of vital signs, laboratory markers (such as lactate), and organ function metrics informs ongoing management, helping to prevent progression to septic shock and to reduce mortality rates.
Balancing Nutrition with Hemodynamic Resuscitation
What are the most effective management strategies for sepsis and septic shock?
Effective management of sepsis and septic shock hinges on early detection and swift implementation of targeted therapies. The cornerstone involves rapid initiation of broad-spectrum antibiotics to eliminate the infectious source. Concurrently, aggressive intravenous fluid resuscitation is vital to restore adequate blood volume and maintain organ perfusion.
If hypotension persists despite fluids, vasopressors—particularly norepinephrine—are employed to stabilize blood pressure. Supportive measures like oxygen therapy, mechanical ventilation, and renal replacement therapy may be necessary depending on the severity of organ dysfunction.
Identifying and controlling the original infection source through diagnostics, surgical intervention, or drainage is crucial. Continuous monitoring of vital signs, lactate levels, and organ function guides ongoing treatment adjustments. These combined strategies aim to halt progression to septic shock, reduce organ damage, and improve survival outcomes.
What role does nutrition play in the management of sepsis?
Nutrition significantly influences recovery in sepsis by addressing the hypermetabolic state characterized by early massive catabolism, muscle wasting, and immune suppression. Adequate nutritional support helps maintain immune competency, supports tissue repair, and preserves lean body mass, which are essential for effective recovery.
In the acute phase of sepsis, early enteral nutrition is preferred because it supports gut integrity, reduces bacterial translocation, and exerts anti-inflammatory effects. It is crucial to tailor nutritional interventions carefully, balancing the need for support with hemodynamic stability, to prevent overload or ischemia.
Nutritional strategies should include addressing micronutrient and vitamin deficiencies, providing approximately 1.0 g/kg/day of protein and moderate non-protein calories (~15 kcal/kg/day). Post-resuscitation, increasing protein intake to 1.5–2.0 g/kg/day and caloric support can help reverse muscle loss and facilitate tissue recovery. Long-term nutritional support with high-protein oral supplements over months to years post-ICU is vital for functional restoration.
What are the common complications associated with TPN in sepsis patients?
Total parenteral nutrition (TPN) in sepsis patients carries several risks. The most significant complication is catheter-related bloodstream infections, which are particularly problematic in immunocompromised or critically ill patients.
Metabolic disturbances frequently observed include hyperglycemia, affecting up to half of patients, and less often hypoglycemia. Liver-related issues such as fatty liver, cholestasis, and fibrosis may develop with prolonged TPN use.
Other complications include hypertriglyceridemia, refeeding syndrome in severely malnourished individuals, and metabolic bone disease over longer durations. Improper line care and aseptic technique increase infection risks, further aggravating patient outcomes.
Why is TPN contraindicated in sepsis?
TPN is generally contraindicated in sepsis patients because it can worsen outcomes. It may promote bacterial growth, especially resistant strains, raising the risk of bloodstream infections. The immunosuppressive effects of TPN and its use via central lines can impair the host's ability to fight infection.
Furthermore, TPN bypasses the gut, leading to mucosal atrophy and increased bacterial translocation, which exacerbates systemic inflammation. Studies show higher resistant bacteria rates in patients receiving TPN, correlating with worse survival.
In contrast, early enteral nutrition maintains gut integrity, supports immune defenses, and reduces infection risk. Therefore, unless enteral feeding is impossible, TPN is avoided to prevent potential aggravation of sepsis.
| Aspect | Details | Implications |
|---|---|---|
| Timing | Early initiation of enteral nutrition in stable patients | Improves outcomes, reduces infection risk |
| Routes | Enteral preferred; TPN when enteral is contraindicated | Gut maintenance, reduced bacterial translocation |
| Micronutrients | Correct deficiencies, support immune system | Enhance recovery, prevent deficiencies |
| Protein & Calories | 1.0 g/kg/day protein; ~15 kcal/kg/day initially | Support muscle mass, match endogenous energy |
| Post-resuscitation | Increase to 1.5–2.0 g/kg/day protein | Reduce muscle loss, improve recovery |
Understanding when and how to use nutritional support can markedly influence the course of sepsis therapy. Prioritizing enteral over parenteral routes, along with individualized targets, helps optimize patient outcomes while minimizing risks.
Clinical Guidelines and Evidence-Based Practices
What are the most effective management strategies for sepsis and septic shock?
Effective treatment of sepsis and septic shock hinges on swift recognition and prompt intervention. The cornerstone approaches include rapid administration of broad-spectrum antibiotics to target the causative infection, coupled with aggressive fluid resuscitation using IV fluids to sustain blood pressure and ensure adequate tissue perfusion. When fluids alone are insufficient, vasopressors—particularly norepinephrine—are employed to maintain stable blood pressure.
Supportive therapies are tailored to individual needs, often requiring oxygen supplementation, mechanical ventilation, or renal support such as dialysis. Crucially, clinicians must identify and eliminate the infection source through diagnostic testing and possible surgical procedures.
Continuous monitoring of vital signs, laboratory indicators like lactate levels, and organ functions guides ongoing treatment decisions. These strategies aim to prevent progression to septic shock, reduce organ failure, and decrease mortality rates.
What role does nutrition play in the management of sepsis?
Nutrition supports the body's response to critical illness by fulfilling increased metabolic requirements and reducing cellular waste. Proper nutritional support helps sustain immune function, preserve muscle mass, and promote tissue repair—all vital for recovery.
Initiating early enteral nutrition (via the gastrointestinal tract) is strongly recommended when the patient is stable and not contraindicated. This approach has been linked with better outcomes, such as fewer infections, shorter ICU stays, and improved survival. In contrast, parenteral nutrition (TPN) is reserved for cases where enteral feeding is impossible or fails, given its associated risks.
Balancing nutritional intake with ongoing resuscitation efforts is essential. Nutritional strategies should be individualized, considering factors like micronutrient needs, protein requirements (~1.0 g/kg/day early on, increased to 1.5-2.0 g/kg/day post-resuscitation), and caloric goals (~15 kcal/kg/day initially). This tailored approach supports immune competence, muscle maintenance, and overall recovery.
What are the common complications associated with TPN in sepsis patients?
While TPN provides essential nutrients when enteral feeding is not feasible, it carries notable risks. Catheter-related bloodstream infections are among the most common complications, often leading to sepsis itself. Such infections can involve resistant bacteria and significantly worsen patient outcomes.
Metabolic disturbances, including hyperglycemia—afflicting up to half of TPN recipients—and hypoglycemia, especially in insulin therapy, are frequent issues. Liver dysfunction is another concern; long-term TPN use can cause fatty liver, cholestasis, and fibrosis.
Other potential adverse effects include hypertriglyceridemia, refeeding syndrome in malnourished patients, metabolic bone disease, and line-related mechanical issues. Ensuring strict aseptic technique and vigilant monitoring minimizes these risks.
Why is TPN contraindicated in sepsis?
TPN is generally contraindicated in sepsis because it may worsen infection severity and outcomes. The infusion of nutrients via central lines can promote resistant bacterial growth, elevating bloodstream infection risks. Studies indicate that non-survivors of sepsis had higher instances of resistant bacteria and longer duration of TPN, suggesting a detrimental role.
Moreover, TPN can suppress the innate immune response, making it harder for the body to combat infection. It may also cause immune suppression by promoting pathogen proliferation and impairing gut mucosal immunity.
Enteral nutrition, which preserves gut integrity and supports immune defenses, is preferred in septic patients. When enteral feeding is impossible, careful assessment is needed, and nutrition should be optimized to avoid the potential exacerbation of sepsis by TPN.
| Aspect | Details | Implications |
|---|---|---|
| Infection risk | Bloodstream infections, resistant bacteria | Avoid TPN unless absolutely necessary |
| Metabolic issues | Hyperglycemia, liver dysfunction | Monitor glucose, liver enzymes |
| Immune system impact | Suppressed immune response | Use enteral nutrition when possible |
| Long-term concerns | Liver fibrosis, metabolic bone disease | Minimize TPN duration |
| Contraindications | Severe infections, intestinal dysfunction | Prioritize alternate routes |
Understanding these aspects ensures clinicians can make informed decisions about nutritional strategies, balancing benefits and potential harms in managing septic patients.
Integrating Nutritional Support within Sepsis Protocols
What are the most effective management strategies for sepsis and septic shock?
Managing sepsis and septic shock effectively hinges on early recognition and swift intervention. The primary goals include promptly administering broad-spectrum antibiotics to eliminate the infection, alongside aggressive intravenous fluid resuscitation to maintain adequate blood pressure and ensure sufficient organ perfusion. When fluids alone are insufficient, vasopressors such as norepinephrine are employed to stabilize circulation. Supportive treatments like oxygen therapy, mechanical ventilation, or renal replacement therapy are tailored to the individual patient's organ failure. Identifying the infection source through diagnostics and surgical procedures helps control the origin of sepsis. Continuous monitoring using vital signs, lactate levels, and organ function tests guides ongoing management, helping prevent progression to septic shock and reducing mortality rates.
What role does nutrition play in the management of sepsis?
Nutritional support is integral to sepsis treatment because it sustains the body during its hypermetabolic state, which involves increased energy expenditure and muscle breakdown. Adequate nutrition helps preserve immune competence, support tissue repair, and prevent further catabolism. It also aids in reducing secondary infections and shortens ICU stays when properly managed. Early initiation of enteral nutrition, when feasible, offers benefits such as preserving gut integrity and reducing bacterial translocation, which is vital in septic patients. Balancing nutritional support with aggressive resuscitation is crucial to avoid complications like fluid overload or gut ischemia. Customized nutritional plans that include sufficient protein, micronutrients, and calories are essential to bolster patient resilience and facilitate recovery.
What are the common complications associated with TPN in sepsis patients?
Total parenteral nutrition (TPN) comes with several risks, especially in septic patients. The most prevalent complication is catheter-related bloodstream infections, which account for a substantial portion of TPN-associated adverse events. Blood glucose levels need close monitoring because hyperglycemia, occurring in up to half of patients receiving TPN, can impair immune response and worsen outcomes. Long-term TPN use may lead to liver complications such as fatty liver, cholestasis, or fibrosis. Metabolic disturbances like hypertriglyceridemia and mineral imbalances are other potential issues. Refeeding syndrome can occur in severely malnourished patients, leading to dangerous shifts in fluids and electrolytes. Ensuring aseptic technique during line management and vigilant monitoring can help mitigate these risks.
Why is TPN contraindicated in sepsis?
In sepsis, TPN is generally contraindicated because it can worsen patient outcomes. It has been linked to increased infection risks, particularly resistant bacteria, contributing to higher mortality in septic patients. TPN may suppress the immune system and increase the likelihood of bloodstream infections due to the necessity of central venous lines. Evidence suggests that enteral nutrition supports gut barrier function and immune defenses better than parenteral routes, reducing bacterial translocation and subsequent infection. The study emphasizes that TPN might even exacerbate sepsis by facilitating resistant infections, which complicate treatment and reduce survival chances. Therefore, whenever possible, nutrition support should favor enteral feeding, reserving TPN for cases where enteral intake is impossible or contraindicated, always with careful risk-benefit analysis.
Optimizing Nutritional Strategies in Sepsis Care
In conclusion, while nutritional support is a cornerstone of sepsis management, the use of TPN warrants cautious consideration due to its associated risks, especially in critically ill septic patients. Early enteral nutrition remains the preferred approach given its role in maintaining gut integrity, reducing secondary infections, and supporting immune function. The current evidence underscores that TPN should generally be reserved for cases where enteral feeding is impossible or contraindicated, and only under strict infection control protocols to prevent complications. Ongoing research into immune-modulating nutrients, the timing of nutritional interventions, and permissive underfeeding offers promising avenues for improving outcomes. Ultimately, individualized nutritional plans integrated seamlessly within sepsis treatment protocols can enhance recovery, reduce complications, and improve long-term prognosis.
References
- Does Total Parenteral Nutrition Increase the Mortality of Patients ...
- NUTRITION THERAPY IN SEPSIS - PMC - PubMed Central
- TPN Contraindications: What You Need To Know
- The Role of Nutritional Support in Sepsis - SpringerLink
- Enhancing sepsis therapy: the evolving role of enteral nutrition
- Septic Shock: Practice Essentials, Background, Pathophysiology
- Nutritional support in sepsis: when less may be more - Critical Care
- Sepsis and Septic Shock - Critical Care Medicine - Merck Manuals
- What are the 2021 pharmacotherapy updates to the Surviving ...