The Impact of Parenteral Nutrition on Patient Recovery
Introduction to Parenteral Nutrition in Clinical Recovery
Parenteral nutrition (PN) is an indispensable medical intervention that sustains patients who are unable to obtain adequate nourishment through oral or enteral means. Its significance extends across various clinical settings, including postoperative recovery, critical care, and long-term treatment scenarios. This article explores the multifaceted impact of parenteral nutrition on patient recovery, examining benefits, risks, clinical guidelines, and recent scientific evidence.
Benefits of Parenteral Nutrition in Patient Recovery

Nutritional support during gastrointestinal failure
Parenteral nutrition (PN) plays a crucial role when patients experience gastrointestinal failure, bowel obstruction, or severe malabsorption, making enteral or oral feeding impossible. It bypasses the digestive system entirely, delivering essential nutrients directly into the bloodstream. This approach ensures patients maintain adequate caloric and protein intake, which is vital for wound healing, tissue repair, and overall recovery.
Patients with conditions such as bowel resection or motility disorders benefit significantly from PN, as it provides a reliable nutritional source during periods when the intestines cannot absorb nutrients effectively. Timely initiation of PN has been shown to improve clinical outcomes, reduce infection risk, and support organ function.
Customization of nutrient composition
One of the major advantages of parenteral nutrition is its flexibility to be tailored to individual patient needs. The nutrient mixture includes carbohydrates, amino acids, lipids, electrolytes, vitamins, and trace elements, adjusted based on factors like weight, disease severity, and metabolic status.
Monitoring laboratory parameters such as blood glucose, electrolytes, and liver function helps optimize PN formulations and avoid complications like hyperglycemia, electrolyte imbalances, or liver issues. For example, in critically ill patients, adding omega-3 fatty acids can reduce inflammation and support organ function.
Support for wound healing and immune function
Proper nutritional support via PN is essential for wound healing, immune response, and overall recovery. Adequate protein supply helps in tissue repair, while vitamins and trace elements bolster immune defenses. In postoperative or trauma patients, PN has been associated with faster wound healing and reduced infection rates.
Recent studies highlight that early and appropriate use of PN can prevent muscle wasting, improve nitrogen balance, and accelerate the return to a healthy nutritional state. These benefits are particularly important in severely injured or immunocompromised patients, where malnutrition can significantly hinder recovery.
| Aspect | Focus | Additional Details |
|---|---|---|
| Indications | When to use PN | Gastrointestinal failure, bowel obstruction, malabsorption |
| Nutrient Tailoring | How nutrients are customized | Based on patient metabolic demands, monitored with labs |
| Patient Outcomes | Benefits | Improved wound healing, immune support, reduced infections |
| Risks and Management | Potential complications | Metabolic disturbances, infections, liver issues, requiring careful monitoring |
Parenteral nutrition remains an indispensable intervention that, when carefully managed, significantly enhances recovery in patients with compromised gastrointestinal function, supporting their healing, immune resilience, and overall clinical progress.
Risks and Complications Associated with Parenteral Nutrition
 Parenteral nutrition (PN) offers vital support for patients unable to meet their nutritional needs orally or enterally, but it carries potential risks that healthcare providers must vigilantly monitor.
Parenteral nutrition (PN) offers vital support for patients unable to meet their nutritional needs orally or enterally, but it carries potential risks that healthcare providers must vigilantly monitor.
One of the most common issues is metabolic disturbances. These include hyperglycemia and hypoglycemia, often resulting from mismatched caloric intake or insulin management. Refeeding syndrome, a serious condition characterized by shifts in fluids and electrolytes, may occur in severely malnourished patients. Moreover, hypertriglyceridemia can develop due to excessive lipid infusion, and electrolyte imbalances are frequent, especially if blood parameters are not closely watched.
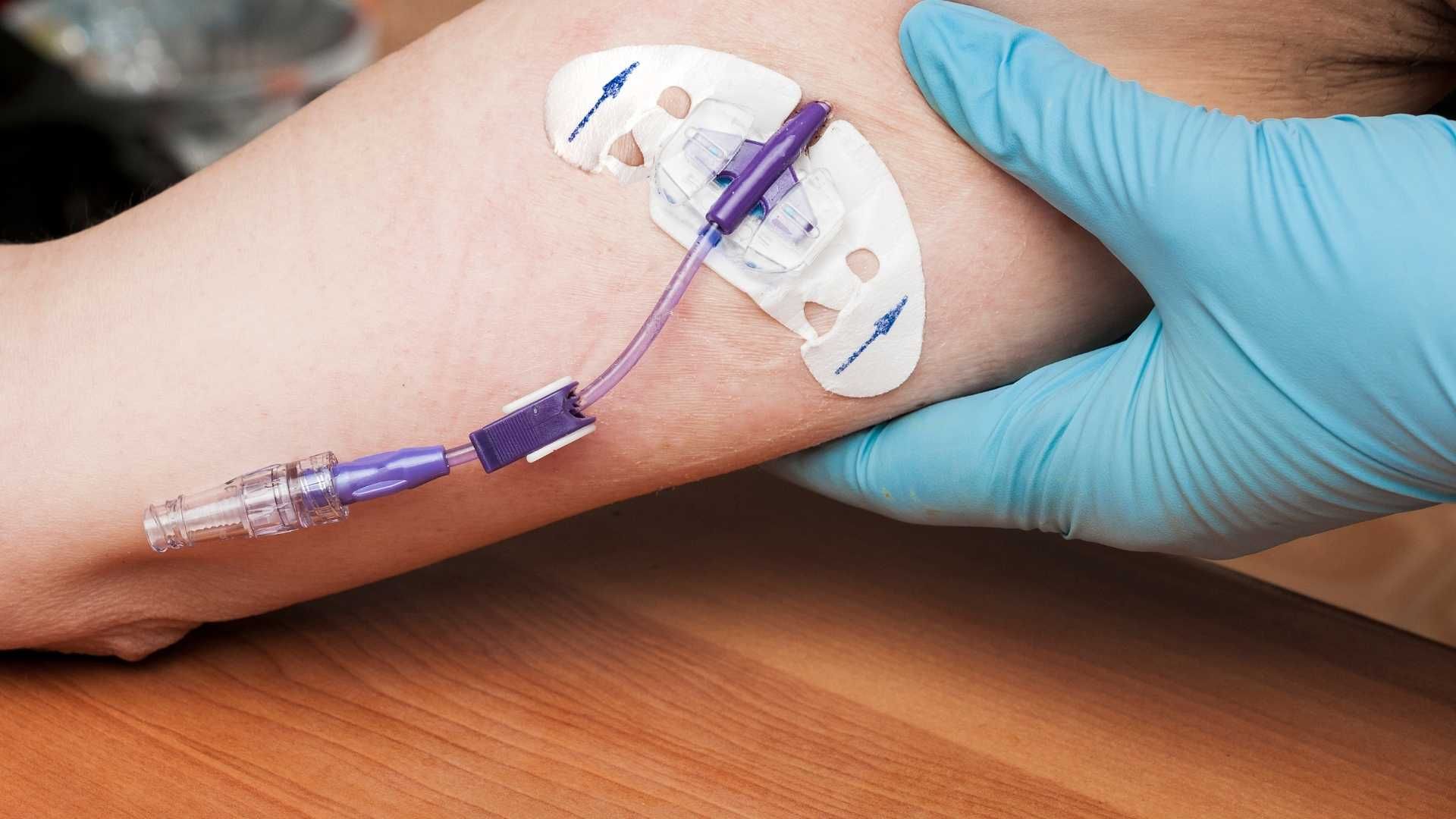
Infectious risks are primarily associated with venous access devices. Catheter-related bloodstream infections, known as CLABSI, pose significant threats, especially with prolonged catheter use. These infections can lead to sepsis and other severe complications. Other local issues include catheter occlusions, thrombosis, and skin infections around the insertion site.
Long-term use of PN can also lead to liver and biliary complications. Fatty liver (hepatic steatosis), cholestasis, fibrosis, and cirrhosis are linked to continuous high lipid administration, bacterial overgrowth, and mineral buildup within the liver. Additionally, sustained PN therapy can result in metabolic bone disease, such as osteoporosis and osteomalacia, influenced by nutritional deficiencies, lack of sunlight, and mineral imbalances.
Monitoring is essential to prevent and manage these adverse effects. Regular blood tests for glucose, electrolytes, and liver function are standard. Proper infection control protocols are critical for vascular access sites. Timely transition to enteral feeding when possible can reduce the duration and risks of PN therapy.
Understanding these potential complications enables clinicians to implement strategies that maximize the benefits of PN while minimizing its hazards, ensuring safer patient outcomes.
Clinical Guidelines for Parenteral Nutrition Administration
What are the clinical considerations regarding calcium and phosphorus in parenteral nutrition?
Proper management of calcium and phosphorus levels in parenteral nutrition (PN) is crucial because imbalanced levels can cause serious complications. A notable risk is the formation of calcium phosphate precipitates, which can block blood vessels or cause pulmonary embolism, potentially leading to fatal outcomes. To prevent this, clinicians must carefully calculate and adjust calcium and phosphorus concentrations, ensuring compatibility within PN formulations. Precise timing and appropriate dosing are essential, especially in patients with mineral imbalances or renal impairment.
Indication criteria for parenteral nutrition
PN is recommended when oral or enteral nutrition is inaccessible or insufficient. Indications include severe bowel obstruction, intestinal failure, high-output fistulas, and significant motility disorders. It is essential that clinical guidelines are followed to justify PN use, focusing on patient-specific needs and nutritional deficits.
Timing of PN initiation
The initiation timing depends on the patient's nutritional status and clinical condition. For severely undernourished or high-risk patients, early PN (within 3–6 days post-surgery) can improve outcomes. Conversely, delaying PN beyond 7 days in stable patients can reduce complications and resource utilization without increasing risks, especially in critically ill individuals. Early initiation supports wound healing and recovery but should be balanced against potential risks.
Vascular access considerations
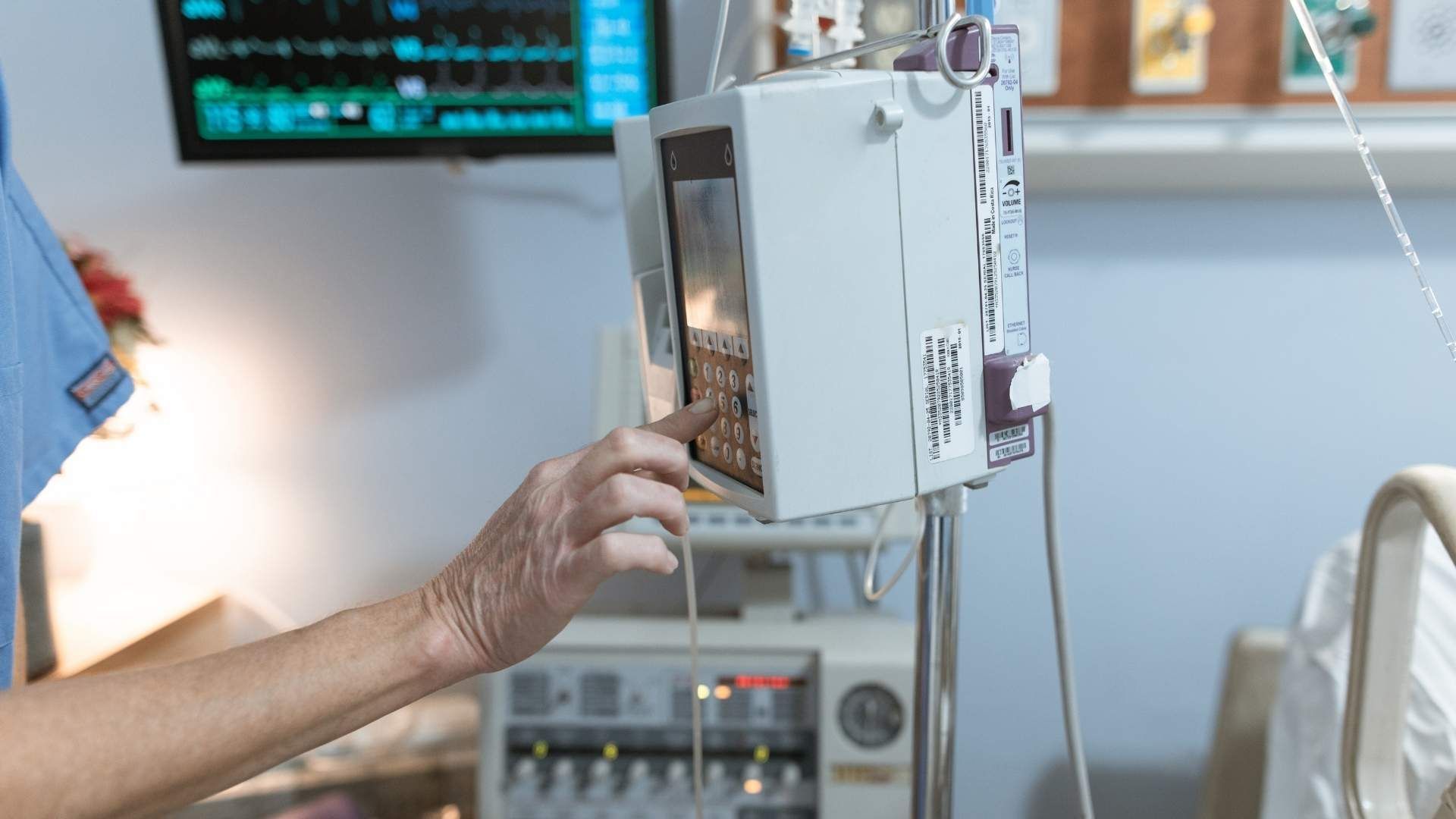
Vascular access choice depends on the PN solution's osmolarity. Hyperosmolar TPN requires central venous access (central lines) to prevent phlebitis or tissue necrosis. For less concentrated solutions, peripheral venous access or midline catheters are options, reducing the risk of complications. Proper placement and maintenance are vital to prevent infections, thrombosis, and mechanical issues. Using tunneled catheters or port devices can minimize infection risks in long-term PN.
Composition and customization of PN formulas
PN formulas should be tailored to meet individual patient needs, considering their caloric requirements, fluid status, organ functions, and disease severity. Typically, they include carbohydrates (dextrose), amino acids, lipids, electrolytes, vitamins, and trace elements. Balancing these components prevents imbalances like hyperglycemia or electrolyte disturbances and accommodates specific conditions such as liver disease or allergies. Advances include lipid emulsions with omega-3 fatty acids and minimal phytosterols to reduce complications like PN-associated liver disease.
Additional considerations
Regular monitoring of electrolytes, blood glucose, liver functions, and nutritional markers is essential during PN therapy. Proper management of calcium and phosphorus, along with vigilant surveillance for metabolic disturbances and infections, can significantly improve patient safety and outcomes.
| Aspect | Key Points | Additional Details |
|---|---|---|
| Indications | Inability to meet nutritional needs enterally or orally | Bowel obstruction, malnutrition, high-output fistulas |
| Timing | 3–6 days for high-risk, after 7 days if tolerated in stable patients | Early for undernourished, delayed for stable patients |
| Vascular access | Central line for hyperosmolar solutions, peripheral for lower osmolarity | Careful placement to avoid infections and thrombosis |
| Formula customization | Include carbs, proteins, lipids, electrolytes, vitamins, trace elements | Balance to prevent complications; adapt based on organ functions and disease |
| Monitoring | Electrolytes, glucose, liver function, nutritional markers | Adjust formulas proactively; prevent metabolic and infectious risks |
Timing of Parenteral Nutrition Initiation in Different Settings
Early versus late initiation in ICU and postoperative cases
The timing of parenteral nutrition (PN) plays a critical role in clinical outcomes for various patient populations. In intensive care units (ICUs), early initiation of PN within the first 24 to 48 hours has traditionally been used for patients unable to meet nutritional needs enterally. However, recent studies, including the EPaNIC trial, demonstrate that delaying PN initiation until after the first week (late PN) can lead to better recovery, fewer infections, and reduced hospital stays.
In surgical contexts, such as post-debulking ovarian cancer surgeries, early postoperative PN has shown mixed results. Some retrospective studies suggest that early PN may prolong recovery and hospital stay, especially in hypoalbuminemic patients. Conversely, strategic delaying of PN, aligned with clinical guidelines, often results in improved outcomes by minimizing complications like infections and delayed bowel function.
Gut rest and early supplementation strategies
The concept of gut rest involves withholding enteral nutrition (EN), typically when bowel function is compromised after surgeries like bowel resection. While gut rest remains necessary in specific cases, early supplementation with supplemental PN can aid recovery by providing essential nutrients without burdening the gastrointestinal tract.
In critically ill patients, early supplemental PN administered within 3–6 days improves nutritional status, reduces energy deficits, and decreases infectious complications. Proper timing ensures that patients receive sufficient calories and amino acids, especially when EN is insufficient or contraindicated. Short-term PN, when carefully monitored, helps maintain cellular functions and supports tissue repair.
Impact on recovery and complication rates
Timing of PN influences both recovery speed and complication risks. Initiating PN too early may increase the risk of metabolic disturbances, infections, and hepatobiliary issues, especially in hypoalbuminemic or malnourished patients. Conversely, delayed PN can help reduce infection rates, organ failure, and length of hospital stay.
Studies consistently indicate that late or delayed PN initiation, particularly beyond the first 7 days of illness or surgery, is associated with fewer infections, shorter ICU and hospital stays, and lower healthcare costs, without adversely affecting mortality. This approach also promotes natural gut function, maintains immune competence, and supports overall recovery.
| Aspect | Early PN Initiation | Late PN Initiation | Additional Notes |
|---|---|---|---|
| Ideal Timing | Within 48 hours post-admission or surgery | After 7 days or longer | Based on patient condition and readiness of gut |
| Benefits | Rapid nutritional support, may prevent muscle loss, early recovery | Reduces risk of infections, organ failure, lowers costs | Especially beneficial in well-nourished, stable patients |
| Risks | Increased metabolic disturbances, infections, hepatobiliary issues | Potential initial energy deficits, delayed recovery | Monitoring key parameters mitigates risks |
| Clinical Recommendations | Use in patients unable to meet nutritional needs enterally early | Preferable in stable, well-nourished patients or where EN is feasible | Tailor timing based on individual patient status |
Understanding the optimal timing for PN initiation helps clinicians improve patient outcomes while minimizing complications. In practice, aligning PN timing with patient-specific factors, clinical guidelines, and recent evidence ensures that nutritional support enhances recovery without introducing preventable risks.
The Role of Parenteral Nutrition in Critical Care and Surgical Recovery

What are the benefits of parenteral nutrition?
Parenteral nutrition (PN) plays a crucial role in patient care, especially when traditional feeding methods are not possible. It provides essential nutrients—calories, proteins, vitamins, and minerals—directly into the bloodstream. This bypasses the digestive system, which might be impaired or inaccessible.
In critically ill or post-surgical patients, PN supports wound healing, immune function, and overall recovery. It is especially beneficial in gastrointestinal conditions such as bowel obstruction, fistulas, or severe malabsorption, where enteral or oral feeding is contraindicated.
Since PN solutions can be customized for each patient, it offers precise nutritional management aligned with individual needs. Proper monitoring during therapy ensures efficacy and minimizes risks.
This intervention can prevent nutritional deficiencies, muscle wasting, and delayed recovery, making it an indispensable tool for managing patients with acute conditions or complex surgery recoveries. However, it requires diligent oversight due to potential complications related to bloodstream infections, metabolic disturbances, and organ-specific issues.
Impact of Timing of Parenteral Nutrition on Recovery Outcomes
How does early versus late initiation of parenteral nutrition (PN) affect recovery in ICU patients?
In critically ill adults, the timing of PN initiation plays a crucial role in patient outcomes. Studies have shown that delaying PN initiation until after day 8 can lead to significant benefits.
Faster recovery and fewer complications are among the most notable advantages of late PN initiation. Patients in late-initiation groups tend to experience shorter durations of ICU and hospital stays.
Specifically, late PN is associated with a decrease in ICU infections, including a reduction in organ failure and inflammatory responses. Additionally, these patients generally require fewer days of mechanical ventilation, which helps reduce the risk of respiratory complications.
Beyond clinical improvements, delaying PN also results in economic benefits. Healthcare costs per patient are notably lower, with a reduction of approximately $1,600. This saving reflects fewer needs for intensive therapies and medications.
Effects on infection, ICU stay, and healthcare costs
Initial stages of critical illness often involve energy deficits that, if unaddressed, can worsen outcomes. Early PN, started within the first 48 hours, has been linked to increased infection rates and longer ICU stays.
In contrast, late PN—initiated after one week—has shown to improve recovery metrics. Patients experience fewer bloodstream and organ-related infections, which are common complications of early aggressive nutritional interventions.
The length of ICU stay drops significantly in late PN groups. This not only benefits patient health by reducing exposure to hospital-related risks but also decreases resource utilization.
Furthermore, cost analyses reveal that late PN reduces overall healthcare expenses. The reduced need for antibiotics, prolonged ICU care, and additional treatments contributes to this cost-effectiveness.
Does delayed initiation lead to quicker recovery?
Yes. Evidence indicates that postponing PN in critically ill patients enhances recovery rates. Patients who start late PN recover faster, with shorter durations of ventilation, ICU stays, and overall hospitalization.
This approach aligns with current guidelines that recommend cautious use of PN, avoiding unnecessary early intervention that may exacerbate inflammation and infections. Instead, early enteral nutrition should be prioritized, with parenteral support reserved for advanced or contraindicated cases.
Overall, the timing of PN significantly influences clinical outcomes, with delayed initiation offering advantages in reducing complications, enabling faster recovery, and lowering costs.
| Aspect | Early PN | Late PN | Impacts |
|---|---|---|---|
| ICU Stay | Longer | Shorter | Faster recovery & less infection |
| Infection risk | Higher | Lower | Reduced bloodstream infections |
| Cost | Higher | Lower | Resource savings |
| Mechanical ventilation | More days | Fewer days | Decreased respiratory complications |
| Mortality | No significant change | No significant change | Similar survival rates |
This data underscores the importance of tailored nutritional strategies, emphasizing late PN initiation to optimize recovery in critically ill and surgical patients.
Comparison of Enteral and Parenteral Nutrition in Patient Recovery
How do clinical outcomes compare between enteral and parenteral nutrition?
Enteral nutrition (EN) is generally preferred because it supports gut function, reduces infection risks, and is associated with better recovery outcomes. Studies indicate that patients receiving early enteral feeding show improved serum protein and albumin levels by days 3 and 5 after surgery, which are markers of better nutritional status.
In contrast, parenteral nutrition (PN), especially when initiated early or systematically, has not demonstrated clear benefits and may sometimes be linked to adverse results. For instance, in critically ill surgical patients, early PN often does not improve, and can even worsen, recovery outcomes compared to delayed or no supplementation.
What are the differences in infection rates?
Infection risk is a major consideration when comparing these two methods. Patients on PN tend to have higher odds of infectious complications such as bloodstream infections, pneumonia, and other sepsis-related issues. For example, one study showed that patients receiving parenteral nutrition had approximately 11 times higher odds of developing pneumonia compared to those on enteral nutrition.
Moreover, the risk of infections like esophageal perforation, diarrhea, and urinary tract infections was also higher in patients on PN. These infection rates significantly impact morbidity and extend hospital stays.
How do hospital stay durations and costs compare?
Patients on parenteral nutrition usually experience longer hospital stays and incur higher treatment costs. Data from large inpatient studies indicate an average increase of about 9 days in hospital stay for those receiving PN compared to enteral feeding.
Financially, parenteral nutrition substantially elevates healthcare expenses. The same studies report that the total costs for patients on PN approximately double those of patients on EN, primarily due to longer intensive care stays, more complications, and the cost of PN solutions.
What are the profiles of complications associated with each?
While both nutrition methods carry risks, PN is more frequently linked with metabolic disturbances such as hyperglycemia, electrolyte imbalances, and liver complications like cholestasis. Infection is a prominent concern, mostly related to venous access devices needed for PN.
Enteral nutrition, when delivered properly, has fewer metabolic complications but can cause issues like feeding intolerance and aspiration risks in some patients.
In summary, optimal recovery is associated with careful selection of nutritional routes. Early initiation of enteral nutrition improves recovery markers and reduces complications, whereas parenteral nutrition, especially if used without strict indications, may lead to increased infection, longer hospital stays, and higher costs.
The Role of Nutritional Status and Preoperative Factors in Recovery

How do albumin levels reflect nutritional reserves and influence recovery?
Albumin levels serve as an indicator of a patient’s nutritional status, particularly reflecting protein reserves. In the context of ovarian cancer patients undergoing debulking surgery, lower preoperative albumin levels (around 2.22 g/dL) were associated with poorer nutritional reserves compared to patients with higher levels (approximately 2.97 g/dL). This deficiency often indicates malnutrition and can impair the body’s ability to recover effectively after major surgery.
Inadequate albumin levels are linked to delayed wound healing, increased susceptibility to infections, and longer hospital stays. They also signal a potential risk for complications, given the body’s reduced capacity for tissue repair and immune function. Therefore, assessing nutritional reserves through albumin levels before surgery is essential for tailoring preoperative nutritional interventions.
What impact does preoperative nutritional status have on surgical and postoperative outcomes?
Patients with compromised nutritional status—especially those with hypoalbuminemia—are more vulnerable to adverse postoperative outcomes. The retrospective study involving ovarian cancer patients found that those on total parenteral nutrition (TPN), often indicative of poorer nutritional reserves, experienced a longer duration until bowel function was restored, averaging 5.77 days versus 4.70 days in better-nourished patients.
Furthermore, these patients faced longer hospital stays (11.46 days compared to 7.14 days), reflecting increased recovery time and resource utilization. The findings suggest that poor preoperative nutritional status can delay recovery, increase the risk of complications, and extend hospitalization.
How does nutrition influence postoperative recovery?
Optimal nutritional management before and after surgery plays a critical role in recovery. Inadequate nutrition impairs immune response, delays tissue repair, and increases complication risks. Conversely, proper preoperative nutrition, especially in malnourished patients, has been shown to improve outcomes.
Proactively addressing nutritional deficits—such as through targeted supplementation—can help restore nutritional reserves, reduce infection rates, and promote faster recovery. This approach is especially important in oncologic and gastrointestinal surgery, where the metabolic demands are high, and malnutrition is prevalent.
| Aspect | Impact of Poor Nutritional Status | Benefit of Adequate Nutrition | Additional Notes |
|---|---|---|---|
| Bowel function recovery | Delayed (e.g., 1+ days longer) | Accelerated recovery | Especially relevant in bowel surgeries |
| Hospital length of stay | Increased (more days, higher resource use) | Shortened hospital stay | Cost-effective outcomes |
| Risk of complications | Elevated risk of infections and wound issues | Reduced complications | Needs proper monitoring |
| Overall recovery | Prolonged and less optimal | Improved, quicker recovery | Involves tailored nutritional strategies |
Summing up
Monitoring and optimizing nutritional status, including preoperative albumin levels, are crucial steps to improve surgical outcomes. Adequate nutrition supports faster bowel function, shorter hospital stays, and fewer complications, ultimately leading to better recovery trajectories for patients undergoing extensive surgeries.
Parenteral Nutrition in Pediatric and Critical Illness Recovery

Pediatric considerations
In pediatric critical care, nutritional support is vital for growth, immune function, and recovery. Enteral nutrition (EN) is generally preferred because it supports gut function and reduces infection risk. However, children often face feeding intolerance, fluid restrictions, or conditions like bowel failure that make EN inadequate.
Parenteral nutrition (PN) becomes necessary when enteral routes cannot meet at least 60% of caloric and protein needs. Proper formulation, including water, carbohydrates, proteins, fats, vitamins, and minerals, must be carefully tailored to each child's age, weight, and clinical status. Postoperative or injury-related malnutrition can delay healing, so timely PN initiation can be life-saving.
Monitoring is essential to avoid complications such as metabolic disturbances, electrolyte imbalances, or liver issues. Regular assessment of serum electrolytes, glucose, and nutritional markers helps optimize therapy.
Metabolic phases in critical illness
Critically ill children experience distinct metabolic phases: the acute (catabolic), stable (transition), and recovery (anabolic) phases.
During the acute phase, high stress and inflammation lead to muscle breakdown and energy depletion. Nutritional strategies aim to prevent further catabolism while supporting vital functions.
In the stable phase, energy expenditure stabilizes, allowing gradual progression toward normal or catch-up growth. Nutritional support should match metabolic needs to avoid overfeeding.
Finally, the recovery phase involves rebuild and repair, where caloric and protein intake should promote tissue regeneration. Tailoring nutrition during these phases improves outcomes, with early enteral feeding supporting gut integrity and immune response.
Avoiding underfeeding and overfeeding
Achieving the right balance in energy provision is critical. Underfeeding can result in muscle wasting, immune suppression, and delayed healing. Excessive feeding, especially hyperglycemia, may cause fatty liver, respiratory burden, and increased mortality.
Using clinical targets, such as 25-30 kcal/kg/day in severe stress or illness and a nitrogen intake of around 1.5 g/kg, guides appropriate calorie and protein delivery. The protein:fat:carbohydrate ratio typically is about 20:30:50% of calories.
Monitoring actual intake versus requirements, adjusting infusion rates, and considering cyclic or intermittent PN help prevent overnutrition. Regular assessment of growth, lab markers, and metabolic parameters ensures optimal nutritional support during pediatric critical care.
| Aspect | Recommendations | Notes |
|---|---|---|
| Timing | Initiate PN within 24-72 hours if enteral feeding is inadequate | Delayed PN can worsen energy deficits |
| Composition | Tailor macro- and micronutrients to child's needs | Include vitamins and trace elements daily |
| Monitoring | Check electrolytes, blood glucose, liver enzymes regularly | Prevent metabolic and hepatic complications |
| Metabolic phases | Adjust nutrition support to acute, stable, and recovery phases | Supports immune function and tissue repair |
| Balance | Prevent under- and overfeeding | Use precise calorie and protein targets |
Optimal use of PN, with vigilant monitoring and timing, is essential for improving recovery outcomes and minimizing complications in pediatric and adult critical illness.
Research Evidence Supporting Parenteral Nutrition Use
 Studies involving 147 ovarian cancer patients who underwent debulking surgery and bowel resection provide valuable insights into the impact of total parenteral nutrition (TPN). The research showed that patients receiving TPN had a longer time until bowel function was restored—averaging 5.77 days compared to 4.70 days with conservative management. Additionally, TPN patients had longer hospital stays, averaging 11.46 days versus 7.14 days for those managed without TPN.
Studies involving 147 ovarian cancer patients who underwent debulking surgery and bowel resection provide valuable insights into the impact of total parenteral nutrition (TPN). The research showed that patients receiving TPN had a longer time until bowel function was restored—averaging 5.77 days compared to 4.70 days with conservative management. Additionally, TPN patients had longer hospital stays, averaging 11.46 days versus 7.14 days for those managed without TPN.
Notably, these patients also showed lower pre-operative albumin levels (2.22 g/dL vs. 2.97 g/dL), indicating poorer nutritional status before surgery. The combined evidence suggests that postoperative TPN may contribute to delayed recovery rather than support it. Especially in hypoalbuminemic patients, TPN was associated with longer recovery times and higher risks of complications.
This growing body of evidence supports clinical guidelines that favor early or enteral nutrition over postoperative TPN in similar surgical contexts. It emphasizes the importance of optimizing nutritional strategies to improve recovery and reduce hospital stay durations.
What does recent research say about the effectiveness of parenteral nutrition?
Recent high-quality studies, including randomized controlled trials, reinforce that initiating parenteral nutrition too early or without clear indications can lead to increased complications, such as infections, and longer hospitalizations. Conversely, delaying TPN when possible or supplementing with enteral nutrition shows benefits like reduced infection rates, shorter ICU stays, and lower healthcare costs.
How does this evidence influence clinical practice?
Clinicians are encouraged to assess nutritional status carefully and prioritize enteral routes when feasible. TPN should be reserved for cases where enteral nutrition is contraindicated or insufficient, particularly considering the potential for delayed recovery and increased complications evident from clinical trials.
Advances in PN Formulations and Clinical Management
How do lipid emulsions and omega-3 fatty acids improve parenteral nutrition?
Recent developments in parenteral nutrition (PN) focus on enhancing formulations to reduce associated complications. Lipid emulsions enriched with omega-3 fatty acids are now being used to improve patient outcomes. These formulations help modulate inflammatory responses and may decrease the incidence of PN-associated liver disease, a common long-term complication.
Including minimal phytosterols, which are plant sterols found in some lipid formulations, can also mitigate liver toxicity. These advances aim to create a more balanced nutrient profile that supports recovery while minimizing adverse effects.
What strategies are important for monitoring and early management?
Proper monitoring is essential during PN therapy. Regular assessment of blood glucose levels, electrolytes, liver function tests, and triglycerides provides critical data to prevent metabolic disturbances.
Early detection of imbalances allows timely intervention. For example, hyperglycemia can be managed with insulin therapy, while electrolyte disturbances require correction to prevent cardiac or neurological issues.
Monitoring protocols should be tailored to each patient, especially those with pre-existing conditions or at high risk of complications.
How do new formulations help reduce long-term complications?
Innovative PN formulations strive to reduce the risk of conditions such as liver cholestasis, fatty infiltration, and bone disease. Lipid emulsions with omega-3 fatty acids have demonstrated anti-inflammatory properties, potentially decreasing organ dysfunction.
Additionally, ensuring that PN solutions contain the appropriate ratios of carbohydrates, proteins, and fats, along with vitamins and trace elements, can optimize recovery and reduce the risk of deficiencies.
Advances in PN also include the development of more stable solutions that minimize the risk of bloodstream infections and metabolic imbalances. Combining these improvements with rigorous monitoring enhances safety and long-term outcomes for patients requiring parenteral nutrition.
Long-term Outcomes and Disparities in Parenteral Nutrition
Parenteral nutrition’s influence on long-term outcomes such as survival and functional status.
Total parenteral nutrition (TPN) can play a crucial role in supporting patient recovery, especially in those with severe gastrointestinal failure or significant malnutrition. When administered appropriately, TPN helps ensure nutritional needs are met, which is vital for wound healing, immune function, and overall strength. Studies suggest that proper management of TPN can improve survival rates and maintain better functional status over the long term.
However, the effectiveness of TPN is not uniform across all patient groups. It heavily depends on factors such as timely initiation, correct formulation, and ongoing monitoring for complications. Risks like infections, liver damage, and metabolic disturbances can impact recovery trajectories if not properly controlled.
Patient populations at risk.
Certain populations are more vulnerable to poorer long-term outcomes related to parenteral nutrition. These include:
- Malnourished patients: Often face increased complications and slower recovery.
- Elderly patients: Tend to have higher rates of comorbidities, affecting their ability to recover.
- Patients with limited healthcare resources: May experience delays in optimal nutritional care due to disparities in access.
- Patients with complex or prolonged gastrointestinal issues: Such as bowel obstruction or high-output fistulas.
Addressing these disparities requires tailored nutritional protocols and ensuring equitable access to advanced nutritional support services.
Addressing disparities and optimizing care
Efforts to improve long-term outcomes involve both clinical and system-wide approaches. Customizing TPN formulations based on individual needs and disease-specific considerations maximizes benefits.
Enhancing healthcare infrastructure to provide equitable access, along with education about timely initiation and proper management of TPN, is essential. Implementing protocols that emphasize early intervention, monitoring, and adjustment of therapy can reduce complications.
Furthermore, ongoing research into formulation improvements—like lipid emulsions with omega-3 fatty acids—aims to minimize long-term liver and metabolic complications, thus supporting better health and functional recovery.
In conclusion, while TPN offers significant benefits for long-term survival and maintaining functional status in severe cases, disparities in access, management, and patient-specific factors must be addressed to optimize outcomes for all.
The Role of Parenteral Nutrition in Managing Special Patient Populations
Providing optimal nutrition is essential for the normal growth, health, and development of children.
In pediatric patients, especially those critically ill, maintaining adequate nutritional status is vital to support growth, immune function, and recovery. During illness, metabolic changes can lead to increased energy and protein needs, but feeding may be compromised due to intolerance or medical contraindications.
In such cases, parenteral nutrition (PN) serves as a critical intervention. It bypasses the gastrointestinal tract, providing nutrients intravenously to meet the patient's requirements. Tailored PN formulas include carbohydrates, amino acids, lipids, electrolytes, vitamins, and trace elements, adapted to each child's condition.
Critical illness recovery
For critically ill adults and surgical patients, early enteral nutrition is generally preferred. However, when enteral feeding is insufficient or contraindicated, early supplemental PN can help prevent energy deficits that worsen outcomes.
Research indicates that initiating PN within 24 to 72 hours in ICU settings can reduce infections, improve muscle mass retention, and support organ function. Conversely, delaying PN until after the first week may promote faster recovery, fewer infections, and lower healthcare costs.
Studies like the EPaNIC trial demonstrated that postponing PN reduces ICU stay, complications, and costs, emphasizing cautious use. Regular monitoring of blood glucose, electrolytes, liver function, and nutritional markers is necessary to prevent metabolic disturbances.
Disparities and healthcare access
Access to appropriate nutritional support varies widely based on healthcare systems, socioeconomic factors, and regional resources. Ensuring equitable provision of PN involves addressing disparities in healthcare access, staff training, and resource availability.
In some regions, limited infrastructure or funding constraints hinder optimal nutritional management, affecting patient outcomes. Education on indications, proper implementation, and monitoring of PN are critical for improving care quality across diverse populations.
Summary table of considerations:
| Patient Population | Indications for PN | Timing of Initiation | Monitoring Focus | Special Considerations |
|---|---|---|---|---|
| Children | Growth, immune support | Early in critical illness if enteral is insufficient | Electrolytes, glucose, vitamins | Adjust formulas for age and weight |
| Adults | Postoperative, ICU support | 24-72 hours if needed, delay if possible | Liver function, metabolic markers | Prevent overfeeding and infections |
| Cancer patients | Malnutrition, treatment support | Based on nutritional assessment | Nutritional status, complication signs | Address unique metabolic demands |
Understanding the nuances of PN use in these populations helps optimize outcomes, minimize complications, and promote recovery.
Summary and Clinical Implications
Parenteral nutrition remains a critical component of patient recovery strategies, especially when enteral routes are contraindicated or insufficient. While its benefits in supporting nutritional needs are evident, the risks and complications necessitate vigilant monitoring and adherence to best practices. Recent research underscores the importance of timing, formulation, and individualized care in optimizing outcomes. Future advancements in PN formulations and protocols promise further improvements in safety and efficacy, ultimately enhancing recovery across diverse patient populations. Clinicians must balance benefits and risks, prioritize evidence-based guidelines, and tailor nutritional strategies to each patient's unique clinical context.
References
- The impact of total parenteral nutrition on postoperative recovery in ...
- Parenteral Nutrition Overview - PMC - PubMed Central
- The Use of Parenteral Nutrition and Disparities in Its Allocation ...
- Parenteral Nutrition: What it Is, Uses & Types - Cleveland Clinic
- Effect of Early vs Late Supplemental Parenteral Nutrition in Patients ...
- Clinical relevance of parenteral nutrition prescription and ...
- Parenteral nutrition in the intensive care unit: cautious use improves ...
- Early versus Late Parenteral Nutrition in Critically Ill Adults
- Total Parenteral Nutrition in the Critically Ill Patient: A Meta-analysis
- The impact of total parenteral nutrition on postoperative recovery in ...