Exploring IDPN solutions for health
Understanding Intradialytic Parenteral Nutrition (IDPN) in Modern Dialysis
Intradialytic Parenteral Nutrition (IDPN) is emerging as a targeted nutritional intervention in the management of malnutrition among dialysis patients. This article explores the mechanisms, benefits, safety concerns, cost implications, and clinical guidelines associated with IDPN, providing a comprehensive overview of its potential to improve patient outcomes in renal health.
Definition and Purpose of IDPN in Dialysis Patients
What is IDPN therapy?
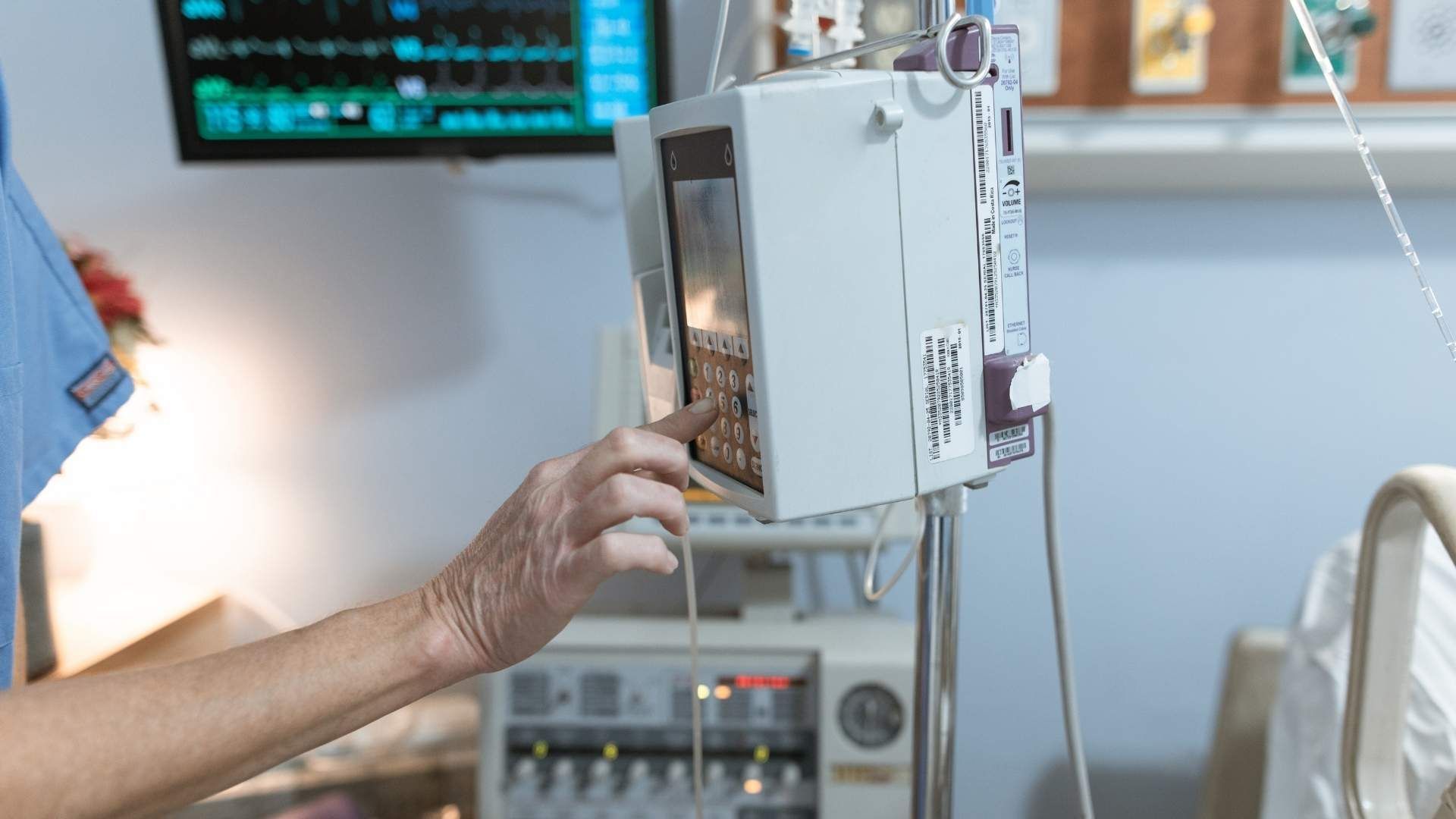
Intradialytic parenteral nutrition (IDPN) is a specialized method of providing nutritional support during hemodialysis sessions. It involves delivering a mixture of essential nutrients—such as amino acids (proteins), dextrose (carbohydrates), lipids (fats), electrolytes, vitamins, and trace elements—directly into the bloodstream via the venous system. This is typically done using infusion pumps at a steady, controlled rate.
The primary aim of IDPN is to combat malnutrition and protein-energy wasting (PEW), common issues in patients with chronic kidney disease undergoing dialysis. These patients often struggle to meet their nutritional needs through oral intake due to factors like taste alterations, nutrient loss during dialysis, inflammation, or dietary restrictions.
Administered over approximately 15 to 30 minutes during dialysis sessions, IDPN requires sterile preparation, proper monitoring, and careful adjustment based on individual patient needs. The therapy is usually recommended for patients who cannot improve their nutritional status with dietary counseling or oral supplements alone.
Despite its capacity to improve certain biochemical markers of nutrition, current research does not conclusively demonstrate that IDPN significantly reduces risks of illness or death. Nonetheless, it remains part of a targeted nutritional strategy, aimed at restoring optimal energy and protein levels to support overall health and potentially improve quality of life.
Indications and patient selection

Who are suitable candidates for IDPN?
Intradialytic Parenteral Nutrition (IDPN) is primarily used for patients undergoing hemodialysis who are malnourished or at risk of malnutrition. Suitable candidates often include patients with severe protein-energy wasting (PEW), indicated by low serum albumin levels, decreased body weight, or poor nutritional intake despite standard treatment.
Patients with chronic kidney disease on dialysis frequently experience nutrient losses and metabolic issues that contribute to malnutrition. When oral and enteral nutrition approaches fail or are contraindicated, IDPN provides an alternative solution. Those with gastrointestinal problems like gastroparesis or severe dietary restrictions are also considered appropriate candidates.
Guidelines on initiating IDPN for malnourished dialysis patients
Current guidelines recommend initiating IDPN only after less invasive nutritional interventions have been tried without success. These include dietary counseling, oral nutritional supplements, and management of underlying conditions.
Healthcare providers are advised to evaluate the patient's nutritional status and potential benefits before considering IDPN. The therapy is generally reserved for patients who have persistent malnutrition, evidenced by low serum albumin, weight loss, or other biochemical markers, and who cannot meet their nutritional needs through oral intake alone.
Particular attention should be paid to the patient’s overall clinical condition, comorbidities, and treatment goals. IDPN should be started under the supervision of a multidisciplinary team including nephrologists, dietitians, and pharmacists.
Assessment parameters before starting IDPN
Before initiating IDPN, comprehensive assessment parameters must be reviewed. These include:
- Serum albumin and pre-albumin levels: Indicative of nutritional status.
- Body weight and BMI: To evaluate weight changes and muscle mass.
- Subjective Global Assessment (SGA): A clinical tool to assess nutritional status.
- Muscle circumference and anthropometry: For muscle mass measurement.
- Laboratory markers: Including cholesterol, triglycerides, and inflammatory markers.
- Assessment of oral intake: Quantity and quality of dietary consumption and reasons for inadequate intake.
- Fluid status and tolerance: To avoid volume overload or electrolyte imbalances.
This detailed evaluation ensures that IDPN is appropriately tailored to the patient’s needs and minimizes risks associated with therapy.
Cost consideration of IDPN
The annual cost of IDPN therapy is approximately $30,000. Given its higher expense compared to oral or enteral nutrition, careful patient selection and regular monitoring are essential to justify its use and assess potential benefits.
SPD (Summary of Patient Selection):
| Criteria | Description | Additional Notes |
|---|---|---|
| Malnutrition or risk factor | Low serum albumin, weight loss, poor dietary intake | Confirmed by clinical and biochemical markers |
| Failure of standard therapies | Ineffectiveness of dietary counseling or oral supplements | After consulting a dietitian |
| Contraindications | Gastrointestinal intolerance, unresponsive to other treatments | Requires multidisciplinary evaluation |
| Monitoring parameters | Serum markers, weight, muscle mass, inflammatory markers | To evaluate therapy effectiveness |
This targeted approach helps optimize the benefits of IDPN while managing costs and risks.
Mechanisms of action and nutritional composition of IDPN
How does IDPN support nutritional status?
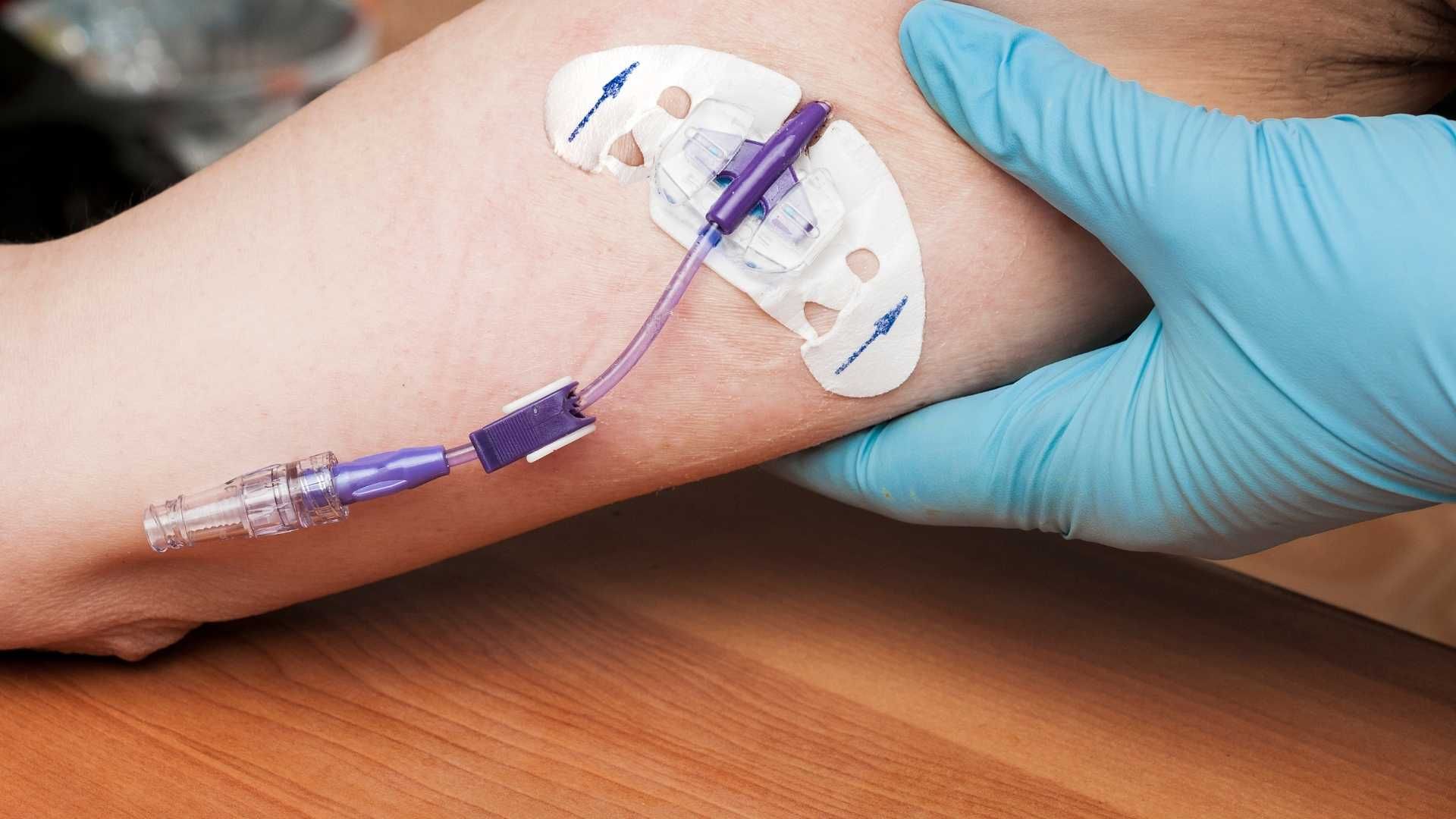
Intradialytic Parenteral Nutrition (IDPN) delivers essential nutrients directly into the bloodstream during dialysis sessions, offering an alternative source of calories and proteins for patients with malnutrition or those who cannot meet their nutritional needs through oral intake alone. By infusing nutrients such as amino acids, glucose, and lipids, IDPN bypasses the gastrointestinal tract, which can be compromised in dialysis patients due to gastroparesis, inflammation, or other health issues. This direct infusion helps improve energy levels, promotes weight gain, enhances muscle mass, and increases serum nutritional markers like albumin and pre-albumin. These changes support better overall health, reduce hospitalizations, and may contribute to improved outcomes in malnourished patients.
Typical composition of IDPN solutions
IDPN solutions are specially formulated mixtures that typically include a combination of amino acids, dextrose, and lipids. These components are usually prepared in three-chamber bags that are ready to use, ensuring standardized administration. For example, a common solution may contain 10% amino acids, providing approximately 4 kcal per gram, along with 20% lipids, offering around 2 kcal/mL, and a specified amount of dextrose, which supplies carbohydrates and calories. The exact composition depends on individual patient needs, guided by nutritional assessment, and can vary significantly.
Customization based on patient needs
Personalized treatment is central to effective IDPN therapy. Healthcare providers, including renal dietitians, assess each patient's nutritional status, baseline serum markers, weight, and oral intake capabilities before customizing the solution. Adjustments can be made in amino acid concentration, lipid content, and glucose amount to meet specific caloric and protein requirements. Patients with more severe protein-energy wasting may require higher amino acid and calorie concentrations, while those with metabolic concerns such as hyperglycemia may need a tailored approach to carbohydrate content. This individualized strategy maximizes nutritional benefits while minimizing risks, making IDPN a flexible tool in managing complex patients.
Potential side effects of IDPN nutrition
While IDPN offers significant benefits, it can also lead to adverse effects such as nausea, vomiting, diarrhea, or infection. Careful monitoring during therapy is essential to identify and address any complications promptly. Proper formulation and administration technique help mitigate these risks, and ongoing assessment ensures the therapy remains safe and effective.
| Aspect | Details | Additional Notes |
|---|---|---|
| Support Mechanism | Direct infusion of amino acids, glucose, lipids | Bypasses gastrointestinal function |
| Composition | Amino acids (protein), dextrose (carbohydrates), lipids | Customizable to patient needs |
| Typical Volumes & Calories | Approximately 900 kcal and 40g protein per session | Based on individual assessments |
| Risks | Hyperglycemia, hypertriglyceridemia, infection | Requires close monitoring |
| Usage Duration | Usually 4-6 months or until goals met | Discontinue once nutritional targets achieved |
For more details on how IDPN supports nutritional mechanisms, further research can be conducted using the term "IDPN nutritional mechanisms." This can provide additional insights into the biochemical and physiological processes involved in IDPN therapy.
Clinical benefits and efficacy evidence
What are the improvements in biochemical markers such as serum albumin?
Intradialytic Parenteral Nutrition (IDPN) has demonstrated some positive effects on nutritional biomarkers in patients undergoing hemodialysis. Several studies reported increases in serum albumin levels, a widely recognized marker associated with mortality risk and nutritional status. For instance, a study observed an average increase of about 0.3 g/dL in serum albumin after three months of IDPN therapy, suggesting an improved protein status.
Serum albumin, along with other markers like transthyretin and pre-albumin, typically reflect the short-term changes in nutritional condition. While these biochemical improvements are encouraging, they do not necessarily translate directly into better clinical outcomes such as reduced mortality or hospitalization rates.
What effects does IDPN have on body weight and muscle mass?
One of the notable benefits of IDPN is its ability to enhance body weight and muscle mass in malnourished hemodialysis patients. Studies have shown increased body weight and improved muscle circumference after several months of treatment. The infusion provides additional calories and protein, which helps reverse muscle wasting and supports overall energy reserves.
In particular, a 3-month IDPN trial indicated significant increases in body weight and muscle mass, which are critical components of nutritional health in dialysis patients. These improvements contribute to better functional status and may reduce the severity of protein-energy wasting (PEW), a common and serious complication in end-stage kidney disease.
How does IDPN impact hospitalization rates and quality of life?
Evidence suggests that IDPN can have a favorable effect on hospitalization rates among malnourished hemodialysis patients. Some studies reported up to a 30% reduction in hospitalizations and a potential 40% decrease in hospital stay duration. These findings imply that improved nutritional status may help prevent complications that lead to hospital admissions.
Despite these positive indicators, comprehensive data on long-term quality of life improvements remain limited. While nutritional improvements are associated with better physical well-being and functional capacity, direct evidence linking IDPN to enhanced quality of life is inconsistent. Current guidelines recommend considering IDPN for specific patients when conventional nutritional interventions have failed, emphasizing that its primary role is supportive rather than curative.
| Effect Area | Observed Change | Additional Details |
|---|---|---|
| Serum albumin | Increased by approximately 0.3 g/dL | Associated with lower mortality risk |
| Body weight and muscle mass | Significant gain after 3 months | Supports functional status and reduces PEW |
| Hospitalization rates | Reduced by around 30% | Shorter hospital stays; potential cost savings |
| Quality of life | Limited direct evidence; improved nutritional status may contribute | More research needed for definitive conclusions |
In summary, while IDPN has shown promising effects on biochemical markers, body composition, and hospitalization rates, the evidence for its impact on survival and quality of life remains less definitive. Its role appears most beneficial when used as part of a targeted nutritional management strategy for malnourished dialysis patients.
Safety profile and adverse effects

What are the common adverse effects and complications associated with IDPN?
Intradialytic Parenteral Nutrition (IDPN) is generally considered safe when administered properly, but like any medical intervention, it carries potential risks. Common adverse effects observed include nausea, muscle pain, and infections such as catheter-related bacteremia. Some patients may experience hyperglycemia, especially if glucose concentrations in the infusion are not carefully managed. Additionally, lipid infusions can lead to hypertriglyceridemia or fatty liver if administered excessively.
Serious complications are rare but can include volume overload, which could worsen hypertension or cause pulmonary edema, and metabolic disturbances like electrolyte imbalances. Though these are infrequent, they highlight the importance of careful patient monitoring.
How are risks monitored and mitigated?
Monitoring strategies are crucial to ensure patient safety during IDPN therapy. This includes regular assessment of blood glucose levels, serum electrolytes, triglyceride levels, and signs of infection. Healthcare providers also watch for symptoms such as swelling, shortness of breath, or fever.
Patients should undergo periodic physical examinations focusing on signs of fluid overload or infections. Blood tests are typically performed at baseline, during therapy, and after completion to detect metabolic abnormalities early.
Adjustments to the composition of IDPN solutions may be necessary based on ongoing monitoring. For example, if hyperglycemia develops, lowering dextrose concentrations or initiating insulin therapy might be required.
What does clinical data say about the safety of IDPN?
Clinical studies generally suggest that IDPN is well tolerated, with no significant increase in adverse events compared to control treatments. In a recent study where IDPN was infused over three months, patients showed increased serum albumin and body weight with no significant adverse effects reported. The safety profile reported in such studies demonstrates that, with proper monitoring, IDPN can be a safe component of nutritional support.
However, it is important to recognize that adverse effects can occur, particularly if therapy is administered without adequate oversight. The risk-benefit ratio needs careful consideration, especially given the costs and limited evidence of clear survival benefits.
By implementing vigilant monitoring strategies and individualizing treatment plans, healthcare providers can maximize the benefits of IDPN while minimizing potential harms. Ongoing research continues to refine safety protocols and patient selection to enhance treatment outcomes.
Guidelines and protocols for administration
Recommended initiation and duration of therapy
IDPN should be considered for malnourished hemodialysis patients when traditional nutritional strategies, like dietary counseling and oral supplements, have proven ineffective or are not tolerated. It is generally started after thorough assessment by a renal dietitian, who considers nutritional markers such as serum albumin, pre-albumin, and Subjective Global Assessment (SGA). The therapy typically continues for 4 to 6 months, with periodic re-evaluation to determine if goals are met or if adjustments are necessary.
The primary purpose of initiating IDPN is to improve the nutritional status of patients with protein-energy wasting (PEW) and severe malnutrition, which are linked to higher morbidity and mortality. Discontinuation is advised once nutritional goals are achieved or if adverse effects such as infections or metabolic disturbances develop.
Preparation, sterilization, and administration procedures
IDPN solutions are usually supplied as ready-to-use three-chamber bags developed by manufacturers like Baxter, containing a balanced mix of amino acids, glucose, lipids, vitamins, and minerals tailored to patient needs. Prior to administration, healthcare providers must verify the correct formulation and ensure compatibility with existing IV access.
Sterile techniques are critical throughout preparation and administration. The solution is infused during the hemodialysis session via a venous drip chamber, using an infusion pump that controls the infusion rate to deliver the prescribed volume, typically around 986 mL per session.
The infusion should be administered over approximately 15 to 30 minutes, aligning with the dialysis session to optimize nutrient delivery and minimize complications. Proper storage and handling of the solutions must follow manufacturer instructions to maintain sterility and stability.
Monitoring and adjustment protocols
Continuous monitoring is essential to ensure safety and efficacy. Patients should be observed for signs of hyperglycemia, infection, or fluid overload. Regular blood tests are required to measure serum albumin, pre-albumin, glucose, triglycerides, and inflammatory markers.
The clinical team, including dietitians and nephrologists, should review nutritional parameters at baseline and periodically during therapy, typically every 4 to 6 weeks. Adjustments to the composition or duration of IDPN may be made based on laboratory results, clinical status, and tolerance.
In cases of adverse effects—such as elevated blood glucose, signs of infection, or hypersensitivity—IDPN should be temporarily discontinued or modified. Discontinuation is generally considered when nutritional goals are achieved or if the patient develops contraindications.
A multidisciplinary approach is recommended, involving careful assessment, tailored formulation adjustments, and close monitoring to ensure optimal outcomes while minimizing risks associated with therapy.
Cost considerations and economic impact
What do we know about cost-effectiveness analyses of IDPN?
IDPN (Intradialytic Parenteral Nutrition) involves delivering nutrients directly into the bloodstream during dialysis sessions. While it shows promise in improving markers such as serum albumin, its implementation is costly compared to standard nutritional interventions like dietary counseling and oral supplements. Several studies have explored its cost-effectiveness, but findings remain inconclusive.
Available analyses suggest that the higher expenses associated with IDPN—due to the need for specialized solutions, infusion equipment, and trained staff—do not always translate into proportionate health benefits. As a result, many health systems are hesitant to universally adopt IDPN, especially given the limited evidence supporting its impact on survival or hospitalization reduction.
How does IDPN compare with other nutritional approaches?
Standard nutritional interventions, including dietary counseling and oral nutritional supplements, are generally less costly and easier to implement. They are first-line strategies recommended by guidelines because they carry fewer risks and are supported by more robust evidence.
IDPN is typically reserved for patients who do not respond to or cannot tolerate these conventional therapies. Because of its expense and the uncertain clinical benefits, healthcare providers often consider IDPN a specialized intervention rather than a routine one.
What are the long-term economic implications?
The long-term economic impact of IDPN is still under investigation. On one hand, if effective, IDPN could potentially reduce hospitalization rates—reported to decrease by up to 30% in some studies—and shorten hospital stays, which would generate cost savings.
However, these savings are counterbalanced by the high costs of the therapy itself and the risks of adverse effects such as infections or metabolic complications. Additionally, if IDPN does not significantly improve survival or quality of life, its financial justification becomes more challenging.
In summary, while IDPN has the potential to improve nutritional markers and reduce some healthcare utilization metrics, current evidence does not firmly establish it as a cost-effective alternative to less expensive nutritional therapies. More comprehensive, long-term economic evaluations are necessary to determine its role in routine clinical practice.
Integration into comprehensive renal nutrition plans
How does IDPN complement other therapies such as dietary counseling?
Intradialytic Parenteral Nutrition (IDPN) is typically considered a supplementary therapy within the broader context of renal nutrition management. It is primarily used for patients who do not respond adequately to conventional treatments like dietary counseling or oral and enteral supplements. Dietary counseling aims to improve nutrient intake through personalized dietary plans, but some patients may experience persistent malnutrition due to issues such as poor appetite, gastrointestinal complications, or metabolic disturbances.
IDPN offers an alternative by providing essential nutrients such as amino acids, glucose, and lipids directly during dialysis sessions. This ensures that nutritional needs are met independently of the patient's appetite or gastrointestinal function, making it especially beneficial for those with severe malnutrition or those unable to tolerate oral intake.
What are the benefits of combining IDPN with other approaches?
Combining IDPN with traditional nutritional strategies can optimize patient outcomes. For example, when used alongside dietary counseling, IDPN can help elevate serum albumin and pre-albumin levels, improve body weight, and enhance energy and protein intake. According to studies, patients receiving IDPN concurrently with nutritional counseling have exhibited significant improvements in their nutritional markers and overall status.
This integrated approach targets different pathways of malnutrition, addressing both intake and nutrient delivery, which can be particularly effective in malnourished patients needing long-term nutritional support.
How does IDPN work together with oral and enteral nutrition?
In cases where patients can tolerate partial oral intake but require additional nutritional support, IDPN can fill the gap. When enteral or oral nutrition alone is insufficient or contraindicated, IDPN provides necessary nutrients during dialysis sessions. This method is especially useful in patients with reduced appetite, gastroparesis, or dietary restrictions.
IDPN solutions are customizable—containing amino acids, glucose, lipids, and trace elements—to meet individual patient needs, complementing oral and enteral nutrition. The goal is to improve biochemical markers, increase body weight, and reverse signs of protein-energy wasting.
A collaborative approach to patient management
Optimal management of malnutrition in dialysis patients involves a team approach, including nephrologists, dietitians, nurses, and pharmacists. This team evaluates nutritional status regularly, selecting suitable therapies like IDPN when standard measures fall short. By integrating IDPN into a comprehensive nutritional plan, clinicians can better address the complex causes of malnutrition, enhance patient quality of life, and potentially reduce hospitalizations.
| Therapy Type | Main Role | Advantages | Limitations |
|---|---|---|---|
| Dietary Counseling | Improve oral intake | Personalized, non-invasive | Not effective in severe malnutrition |
| Oral/Enteral Supplements | Boost nutrient intake | Easier administration | Tolerance issues, gastrointestinal problems |
| IDPN | Direct nutrient infusion during dialysis | Bypasses GI issues, tailored formulations | Higher cost, potential risks |
This multi-modal strategy ensures a comprehensive approach to nutritional health in dialysis patients, aligning therapies to patient needs and maximizing outcomes.
Implementation in different clinical settings
Use of IDPN in hospital and outpatient settings
In hospitals, Intradialytic Parenteral Nutrition (IDPN) is often administered during supervised dialysis sessions. Healthcare providers such as nephrologists, dietitians, and nurses collaborate to tailor the nutrient solutions based on individual patient needs, focusing on malnourished patients who do not respond well to oral or enteral nutrition. Outpatient clinics follow similar protocols, ensuring proper infusion during scheduled dialysis sessions.
IDPN can improve nutritional markers and increase body weight, which is vital for patient recovery and overall health. Its controlled environment in hospitals facilitates close monitoring for any adverse effects, including infections or metabolic disturbances.
Use in community dialysis units
Community dialysis units are increasingly adopting IDPN for patients who experience severe malnutrition but prefer or need dialysis outside hospital settings. For successful implementation, these units must have the necessary infrastructure, including infusion pumps, pharmacy support for preparing customized solutions, and trained staff to manage treatments.
Ensuring patient safety requires adherence to protocols for administering IDPN, monitoring biochemical parameters, and watching for complications like hyperglycemia or fluid overload. When properly managed, community-based IDPN can help maintain better nutritional status over the long term, reducing hospitalizations and improving quality of life.
Criteria for setting up IDPN programs
Establishing an IDPN program involves several criteria to ensure safety and efficacy. First, a thorough nutritional assessment by a renal dietitian must confirm the need for supplemental parenteral nutrition. The program requires access to licensed, ready-to-use solutions, preferably in multi-chamber bags, which simplify preparation and dosing.
Facilities should have appropriate infusion equipment and trained personnel skilled in infusion therapy. Staff must be capable of monitoring for side effects like infections, metabolic imbalances, and volume status. Having pharmacy support and proper documentation protocols is also essential.
Additionally, institutions should follow guidelines recommending IDPN primarily for patients unresponsive to or intolerant of oral or enteral nutrition, emphasizing safety, cost-effectiveness, and patient-specific considerations. Regular review and reassessment are necessary to determine the continuation or discontinuation of therapy based on treatment response and goals.
Summary of implementation criteria in a tabular format:
| Setting | Infrastructure Needed | Staff Qualifications | Monitoring Focus | Typical Duration |
|---|---|---|---|---|
| Hospital | Infusion pumps, pharmacy support, safety protocols | Trained nephrologists, nurses, dietitians | Biochemical parameters, adverse events | 4-6 months, or as long as needed |
| Outpatient clinics | Similar to hospital, with community support systems | Trained dialysis staff, dietitians | Nutritional markers, complications | Depending on patient needs |
| Community units | Proper infusion equipment, trained personnel | Trained staff in infusion management | Hyperglycemia, infection, fluid status | As per individual treatment plan |
Implementing IDPN tailored to the setting and patient needs can significantly enhance nutritional support and potentially improve outcomes for dialysis patients.
Research gaps and future directions
Understanding the full benefits and limitations of Intradialytic Parenteral Nutrition (IDPN) is essential for optimizing care in hemodialysis patients. Currently, much of the evidence is derived from small or short-term studies, leaving significant gaps regarding its long-term impact on survival and quality of life. There is a pressing need for large-scale, prospective research that can conclusively determine whether IDPN offers survival advantages or reduces hospitalization rates.
One promising area is the potential for personalized nutritional therapy. Since patients vary widely in their nutritional needs, metabolic responses, and comorbidities, tailoring IDPN solutions to individual profiles might improve effectiveness. Customization could involve adjusting amino acids, glucose, lipids, and micronutrients based on biomarkers such as serum albumin, pre-albumin levels, and body composition measurements.
Emerging technologies hold promise for advancing IDPN practice. Innovations in formulation, including formulations combining novel nutrient delivery systems or bioactive compounds, could enhance patient outcomes. Additionally, improved infusion devices and monitoring systems could optimize administration, reduce risks, and facilitate real-time adjustments. Further research into these technological advances may lead to more efficient and safer nutritional support.
Future research should also evaluate the cost-effectiveness of personalized approaches and technological innovations in IDPN. Comparing these strategies to standard care can help determine their practical viability and potential integration into clinical practice. By closing these gaps with robust data, clinicians can better identify which patients are most likely to benefit from IDPN and how to implement it safely and effectively in diverse settings.
In summary, advancing our understanding of IDPN requires studies focusing on long-term outcomes, personalized treatment plans, and leveraging new technologies. Such efforts will be key to transforming IDPN from a therapy of uncertain benefit to a tailored, evidence-based standard for managing malnutrition in hemodialysis patients.
Summary and conclusions
What are the main takeaways regarding the effectiveness and safety of IDPN?
Intradialytic Parenteral Nutrition (IDPN) is designed to support malnourished patients undergoing hemodialysis by delivering essential nutrients directly during dialysis sessions. The evidence indicates that IDPN can improve some nutritional markers, such as serum albumin, weight, and muscle mass. Studies, including randomized controlled trials, show that IDPN generally increases energy and protein intake, with some patients experiencing better wound healing and subjective health assessments.
However, despite promising improvements in biochemical markers and nutritional status, clear benefits in reducing mortality or hospitalization rates have not been conclusively demonstrated. The safety profile appears acceptable overall, with no significant difference in adverse events reported compared to standard care, although risks like infection, hyperglycemia, and fluid overload are considerations.
What are the current clinical recommendations?
Current guidelines suggest using IDPN primarily as a secondary intervention for patients who do not respond adequately to dietary counseling and oral supplementation. It should be considered when nutritional status fails to improve with standard options, especially in cases of severe protein-energy wasting (PEW). Before initiating IDPN, a thorough assessment by a renal dietitian is essential, and therapy should ideally be tailored to the individual’s needs.
IDPN is recommended for short to medium-term use, typically 4–6 months, with discontinuation once nutritional goals are met or adverse effects arise. Routine monitoring is critical to ensuring safety, and therapies should be reviewed regularly.
What is the outlook for nutritional management in dialysis patients?
The future of nutritional management in dialysis includes exploring more personalized approaches, such as customized nutrient formulations and advanced monitoring tools. While IDPN remains a valuable option for select patients, ongoing research aims to clarify its long-term benefits and cost-effectiveness.
Improving overall nutritional strategies, including better integration of oral, enteral, and parenteral options, alongside developments in low-cost formulations and safer delivery methods, might enhance outcomes. Advances in understanding inflammation, metabolic disturbances, and individual variability will likely shape more effective, personalized nutritional interventions in the dialysis population.
Concluding Perspectives on IDPN in Dialysis Care
While IDPN presents a promising approach to tackling malnutrition in dialysis patients, its use must be carefully individualized, considering both its clinical benefits and limitations regarding safety and cost. Current guidelines support its application in specific patient subgroups, but further research is essential to establish definitive benefits in survival and quality of life. As innovations in nutritional solutions continue, IDPN's role is likely to evolve, emphasizing personalized, multidisciplinary kidney health management.
References
- Intradialytic Parenteral Nutrition - an overview | ScienceDirect Topics
- Nephrology - Clinical Nutrition EMEA - Baxter
- Intradialytic Parenteral Nutrition - an overview | ScienceDirect Topics
- Evidence Brief: Use of Intradialytic Parenteral Nutrition (IDPN ... - NCBI
- Exploring the Options for Peritoneal Dialysis - Patient Care America
- The beneficial effects of intradialytic parenteral nutrition in ... - Nature
- (PDF) Evidence Brief: Use of Intradialytic Parenteral Nutrition (IDPN ...