Potential Complications of Total Parenteral Nutrition and How to Manage Them
Understanding the Risks of Total Parenteral Nutrition (TPN) for Better Outcomes
Total Parenteral Nutrition (TPN) is a vital intervention for patients who cannot meet their nutritional needs through conventional oral or enteral routes. Despite its lifesaving benefits, TPN carries a range of potential complications that can impact patient outcomes if not carefully managed. This article explores the common and severe adverse effects associated with TPN, their underlying causes, and strategies for effective prevention, early detection, and management to optimize patient safety and treatment efficacy.
Common TPN-Related Complications and Their Clinical Significance
What are the most common complications associated with total parenteral nutrition (TPN)?
Total parenteral nutrition (TPN) offers lifesaving nutritional support for patients unable to consume or absorb food normally. However, it carries a range of complications that healthcare providers must vigilantly monitor and manage.
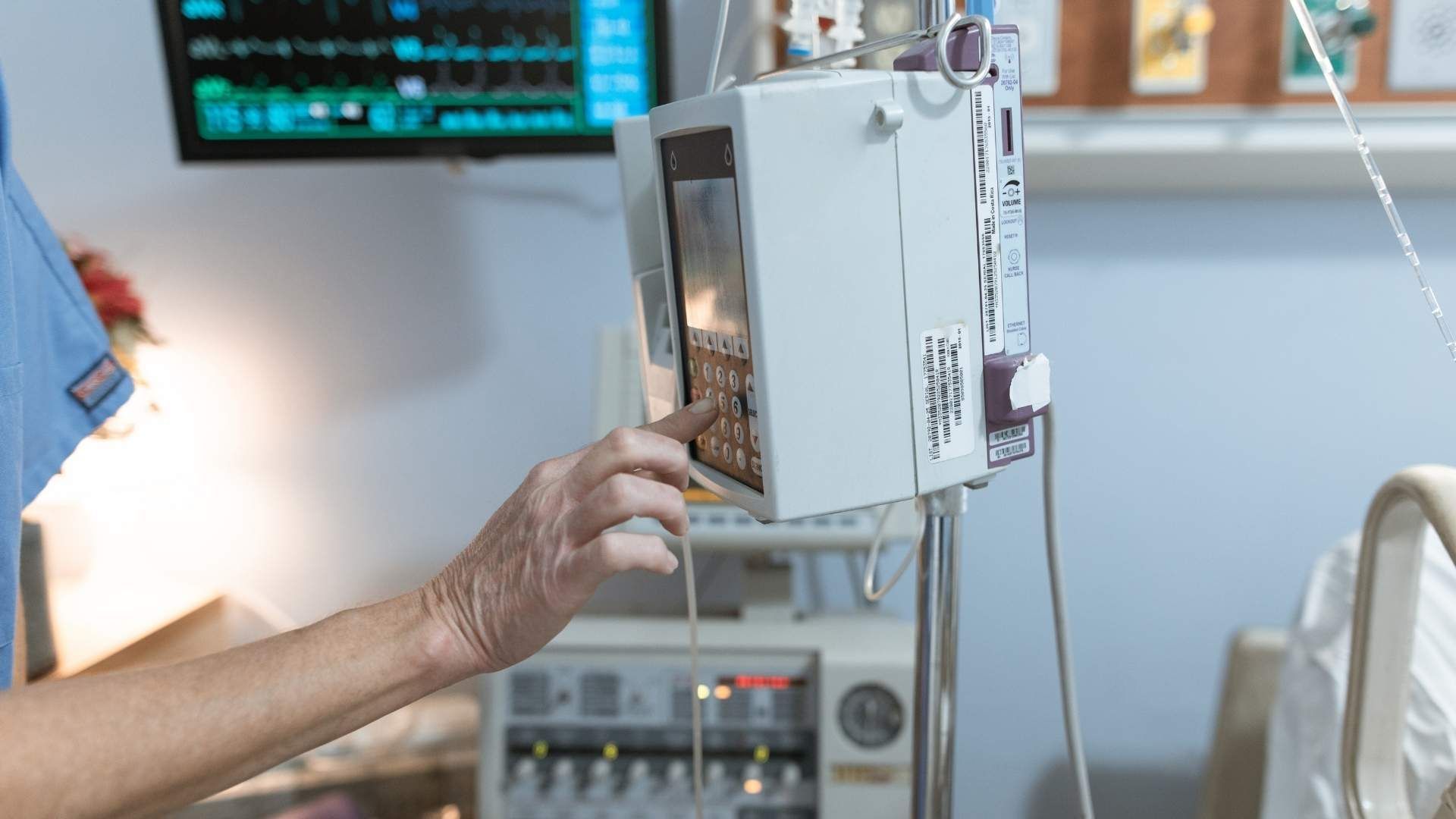
One of the most frequent challenges is metabolic disturbances. These include hyperglycemia, which occurs in up to 50% of patients on TPN, especially among those with insulin resistance, diabetes, or those receiving steroids. Managing blood glucose levels with insulin adjustments and frequent monitoring is critical. Conversely, hypoglycemia can happen if TPN is abruptly interrupted, requiring careful titration and adjustments.
Electrolyte imbalances are common, affecting about 90% of TPN recipients. These include hypophosphatemia, hypokalemia, hypocalcemia, and hypomagnesemia, which can lead to serious consequences like arrhythmias, muscle weakness, or neurological disturbances. Refeeding syndrome is a particularly severe form of electrolyte shift that can occur within 24 to 48 hours of initiating refeeding, especially in severely malnourished patients. Prevention relies on gradual nutritional repletion and close electrolyte monitoring.
Hypertriglyceridemia, found in 25-50% of patients, can also be problematic. Elevated triglyceride levels (>1000 mg/dL) may induce pancreatitis and impair microcirculation, necessitating lipid intake adjustments.
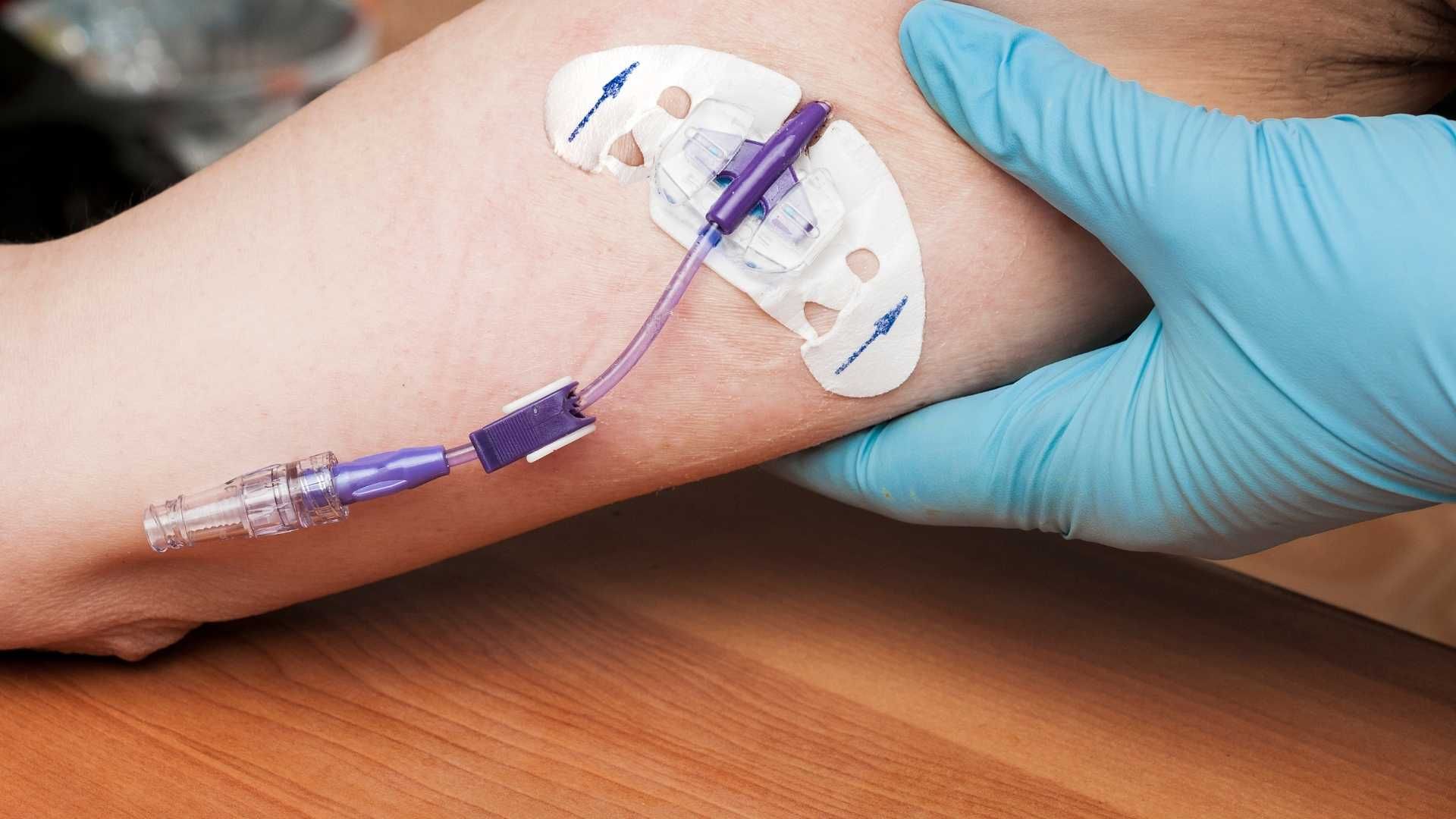
In addition to metabolic issues, infection risks are significant. Catheter-associated bloodstream infections, such as central line-associated bloodstream infections (CLABSI), pose severe threats, potentially leading to sepsis. Strict aseptic technique during catheter insertion and maintenance, routine site inspection, and regular line flushing are essential preventive measures.
Local infections at the catheter site, air embolisms, pneumothorax, and venous thrombosis are mechanical line complications associated with insertion and maintenance. Proper insertion techniques, post-insertion chest X-rays, and vigilant line care help minimize these risks.
Long-term TPN use, especially in home settings, increases the risk for hepatobiliary and bone-related issues. Hepatic complications include fatty liver (steatosis), cholestasis, and, in some cases, progression to fibrosis and cirrhosis. These are often precipitated by overfeeding, especially excess lipids or carbohydrates, and recurrent infections. Management strategies involve modifying lipid formulations—using omega-3 fatty acids or medium-chain triglycerides—and limiting caloric overload.
Bone disease, affecting about 40% of long-term TPN patients, manifests as osteoporosis or osteomalacia. Deficiencies in calcium, phosphate, and vitamin D contribute, and treatment includes supplementation and medications like bisphosphonates.
Overall, the spectrum of TPN complications underscores the importance of comprehensive patient monitoring, early detection, and intervention. Routine assessments include serum electrolytes, blood glucose levels, liver function tests, and bone mineral density evaluations. Adhering to best practices in catheter care, nutritional formulation, and metabolic management can significantly reduce adverse outcomes and improve patient safety.
Metabolic Complications: Hyperglycemia, Electrolyte Imbalances, and Refeeding Syndrome
What is the pathophysiology behind hyperglycemia, electrolyte disturbances, and refeeding syndrome in TPN?
Total parenteral nutrition (TPN) delivers nutrients directly into the bloodstream, which can cause various metabolic disturbances. Hyperglycemia occurs primarily due to an excess of glucose infused through TPN, especially in insulin-resistant patients, such as those with diabetes or those receiving steroids. The high glucose load overwhelms the body's ability to utilize insulin effectively, leading to elevated blood sugar levels.
Electrolyte imbalances are common because refeeding, particularly in severely malnourished patients, causes rapid shifts of electrolytes like phosphate, potassium, and magnesium into cells. During refeeding syndrome, insulin secretion increases in response to carbohydrate intake, causing cellular uptake of these electrolytes, which can precipitate deficiencies in the bloodstream.
Refeeding syndrome results from sudden shifts in fluids and electrolytes, leading to severe hypophosphatemia, hypokalemia, and hypomagnesemia. This syndrome mainly affects malnourished individuals reinitiating nutrition, with potential complications including arrhythmias, muscle weakness, and neurological symptoms.
What are the clinical manifestations of these metabolic disturbances?
Hyperglycemia presents with symptoms like increased thirst, frequent urination, and fatigue. If poorly managed, it can lead to dehydration, ketosis, or diabetic ketoacidosis.
Electrolyte disturbances often manifest as muscle weakness, cramps, arrhythmias, or neurological symptoms such as confusion or seizures when severe deficiencies occur.
Refeeding syndrome's symptoms include behavioral changes, muscle weakness, respiratory failure, seizures, and cardiac arrhythmias due to electrolyte imbalances and fluid overload.
These complications may develop within 24 to 48 hours of initiating or reinitiating TPN in at-risk patients.
How can these complications be managed effectively?
The cornerstone of management involves careful monitoring and gradual initiation of PN:
- Start TPN slowly, especially in malnourished patients, to allow gradual metabolic adaptation.
- Regularly monitor blood glucose, electrolytes (phosphate, potassium, magnesium), and acid-base status.
- Use insulin therapy to manage hyperglycemia, adjusting doses based on blood sugar levels.
- Correct electrolyte deficiencies promptly with supplemental electrolytes, typically intravenously.
- Avoid rapid infusion rates and provide electrolyte replenishment before and during TPN administration.
- Engage in close clinical monitoring for symptoms of refeeding syndrome, including vital signs and neuromuscular assessments.
- In cases of severe electrolyte imbalance, consider temporary cessation or modification of TPN until stability is achieved.
By implementing these strategies, healthcare providers can minimize the risk of these potentially life-threatening complications, improving patient outcomes during TPN therapy.
Infection Risks and Strategies for Prevention
How can TPN complications be prevented and managed effectively?
Preventing complications in patients receiving total parenteral nutrition (TPN) is vital to improve outcomes and reduce mortality. Key strategies include meticulous monitoring and strict adherence to protocols.
Regular blood tests are essential for early detection of potential problems. These tests typically include checking serum electrolytes, liver function, triglyceride levels, and markers of infection. Continuous monitoring helps in timely identification and correction of abnormalities.
Electrolyte disturbances such as hypokalemia, hypophosphatemia, and hypomagnesemia are common during initiation and require prompt supplementation. Liver function tests, performed at least weekly, detect early signs of hepatic stress or damage—particularly important during long-term TPN.
Monitoring triglyceride levels is crucial to prevent severe hypertriglyceridemia, which can cause pancreatitis and affect microcirculation. Adjusting lipid formulations and infusion rates based on these results helps avoid complications.
Active management involves adjusting the TPN formulation tailored to each patient's needs—ensuring an appropriate balance of macronutrients and micronutrients.
Strict adherence to aseptic techniques during catheter insertion, maintenance, and dressing changes dramatically reduces infection risk. This includes hand hygiene, using sterile gloves and drapes, proper skin disinfection, and avoiding line manipulations unless necessary.
Detection of infections such as catheter-related bloodstream infections (CRBSI) involves blood cultures drawn simultaneously from the line and peripheral veins. Recognizing early signs like fever, chills, or hypotension prompts urgent investigation.
Responding swiftly to suspected infections is crucial. The infected catheter should be removed if blood cultures are positive, and appropriate antimicrobial therapy should begin immediately.
Prevention strategies extend to regular inspection and maintenance of the catheter site, minimizing lumens, and using antimicrobial-impregnated dressings when appropriate.
Overall, a multidisciplinary approach involving physicians, nurses, and pharmacists ensures rigorous infection control, appropriate nutritional management, and early intervention, significantly reducing TPN-related complications.
Topics Covered
| Topic | Details | Additional Information |
|---|---|---|
| Catheter-Related Bloodstream Infections | Central line infections (CRBSI) are common and serious | Blood cultures, removal, antibiotics, aseptic line care |
| Aseptic Techniques | Critical for line insertion and maintenance | Hand hygiene, sterile gloves, disinfection routines |
| Detection and Response | Early signs include fever and hypotension | Blood cultures, prompt removal, and targeted therapy |
This comprehensive approach safeguards the patient from severe infections and other complications associated with TPN, ensuring safer nutrition therapy.
Monitoring Protocols for Early Detection of TPN Complications

What monitoring protocols are recommended for early detection of TPN-related complications?
Effective management of patients receiving total parenteral nutrition (TPN) hinges on meticulous and regular monitoring to identify potential complications before they become severe. Standard protocols involve frequent assessment of laboratory parameters, vigilant clinical evaluations, and close observation for signs of infection and metabolic instability.
Laboratory tests play a critical role in early detection. Regular blood glucose measurements are necessary, especially for patients with insulin resistance or those at risk of hyperglycemia or hypoglycemia. Serum electrolytes, including sodium, potassium, calcium, magnesium, and phosphate, should be checked daily during the initial phase and as clinically indicated thereafter. These help identify electrolyte disturbances such as hypophosphatemia, hypokalemia, hypocalcemia, and hypomagnesemia, which are common and can have serious consequences.
Liver function tests are essential, especially for long-term TPN patients, to monitor for hepatic complications like fatty liver or cholestasis. Triglyceride levels should be measured regularly, particularly if lipid emulsions are part of the TPN formula, to detect hypertriglyceridemia that can lead to pancreatitis or microcirculatory issues. Markers of bone health, including serum calcium, phosphate, alkaline phosphatase, and vitamin D levels, should be monitored periodically to prevent and manage metabolic bone disease.
Clinical assessments are equally important. Close observation of catheter sites for redness, swelling, discharge, or signs of local infection can prevent bloodstream infections. Daily checks of the insertion site and adherence to aseptic techniques are vital. Symptoms such as fever, hypotension, or new-onset chills should prompt immediate investigation for bloodstream infections, including blood cultures from the catheter and peripheral sites.
Monitoring fluid status is crucial for detecting overload or dehydration. This involves tracking intake and output diligently, weekly weighing, and monitoring vital signs regularly. Signs of pulmonary edema, such as dyspnea or crackles on auscultation, require prompt intervention.
The frequency of these assessments varies depending on the patient's stability. During initial stabilization, testing may be required daily, whereas stable patients might be monitored less frequently—every 2-3 days or weekly with adjustments based on clinical evolution.
In summary, a comprehensive monitoring strategy incorporating laboratory analysis, clinical evaluation, and infection surveillance is essential. This proactive approach not only detects complications early but also guides timely interventions, ultimately improving patient outcomes in TPN therapy.
Factors Increasing the Risk of TPN-Related Adverse Effects
What factors increase the risk of adverse effects from TPN?
Parenteral nutrition (PN), especially total parenteral nutrition (TPN), is a complex therapy that carries potential risks. Several factors contribute to the likelihood of developing complications during TPN therapy.
Patient-related factors play a significant role. Individuals with pre-existing liver disease are more prone to develop hepatic complications such as fatty liver, cholestasis, and fibrosis. Those with metabolic disorders or immunosuppression are at increased risk for infections and metabolic imbalances. Electrolyte imbalances before starting TPN can predispose patients to severe disturbances when nutrition is initiated.
Technical and procedural issues are critical determinants of safety. Poor sterile technique during catheter insertion and maintenance increases the risk of bloodstream infections, including catheter-related bloodstream infections (CLABSI). Improper line placement or inadequate site care also elevate risks of thrombosis, pneumothorax, air embolism, and vascular injury. Ensuring strict aseptic practices, proper line management, and correct insertion protocols minimizes these risks.
The duration of TPN therapy influences complication rates as well. Long-term use, often extending beyond several months, is associated with hepatic dysfunction, cholestasis, metabolic bone disease, and micronutrient deficiencies. The cumulative effect of prolonged infusions necessitates vigilant monitoring of liver function, bone health, and micronutrient status to mitigate these adverse outcomes.
Inadequate monitoring and administration errors further enhance the risk profile. Rapid infusion of glucose or excessive carbohydrate loading can cause hyperglycemia or hypoglycemia upon abrupt cessation. Fluctuations in electrolyte levels, if not promptly corrected, can lead to severe complications such as refeeding syndrome, arrhythmias, or neuromuscular disturbances.
Additional factors include improper formulation of PN, such as unbalanced macronutrients or excess trace elements like manganese, which may induce toxicity or metabolic disturbances. Infusion-related issues like line blockage, thrombosis, or occlusions can interrupt therapy and cause additional morbidity.
To prevent these complications, comprehensive patient assessment before initiating TPN, meticulous line insertion and maintenance techniques, routine laboratory monitoring, and individualized PN formulations are essential. Educational programs for healthcare staff and adherence to strict infection control protocols significantly reduce the incidence of adverse effects.
In summary, a combination of patient-specific vulnerabilities, technical challenges during line placement, and long-term management issues collectively heighten the risk of TPN-related complications. Tailoring therapy, rigorous monitoring, and adherence to best practices are vital to minimize these risks and ensure safe nutrition support.
Clinical Implications of TPN-Related Complications
What are the clinical implications of TPN complications for patient health?
Parenteral Nutrition (PN), especially Total Parenteral Nutrition (TPN), is an essential therapy for patients who cannot meet their nutritional needs orally or enterally. However, it carries considerable risks that can significantly impact overall health.
One of the most serious outcomes of TPN complications is increased morbidity and mortality. Infections, particularly bloodstream infections such as catheter-related bloodstream infections (CRBSI), are among the most common and life-threatening. These infections, if not promptly detected and managed, can lead to sepsis, multiple organ failure, and even death. Vascular injuries like pneumothorax, air embolism, and thrombosis also pose immediate life-threatening risks.
Metabolic disturbances are another major clinical concern. Hyperglycemia, electrolyte abnormalities like hypophosphatemia and hypokalemia, and refeeding syndrome can impair organ functions, cause cardiac arrhythmias, muscle weakness, seizures, and respiratory failure. Hepatic toxicity, including cholestasis and fatty liver, can develop after long-term TPN use, further deteriorating liver function and risking progressive liver failure.
Bone health is also compromised over time, with long-term PN patients experiencing osteomalacia and osteoporosis due to deficiencies in calcium, phosphate, and vitamin D. These conditions increase fracture risk and can cause chronic pain, reducing physical mobility and quality of life.
Long-term complications extend to micronutrient imbalances, which may lead to vitamin and mineral deficiencies, impacting immune function, wound healing, and neurological health.
The cumulative effect of these complications results in prolonged hospital stays, increased healthcare costs, and a significant decline in patient quality of life. Patients may suffer from chronic pain, reduced mobility, dependence on long-term medical care, and psychological stress.
Effective management involves routine monitoring of blood parameters, strict adherence to aseptic techniques, timely treatment of infections, and individualized adjustment of PN formulation. Early detection and intervention are vital to prevent escalation into severe organ dysfunction or death.
In summary, the clinical implications of TPN complications emphasize the importance of vigilant care, comprehensive monitoring, and proactive strategies to mitigate risks. This approach is essential to improve survival rates, preserve organ function, and enhance the overall well-being of patients reliant on TPN therapy.
Best Practices for Safe TPN Administration and Complication Reduction
What are the best practices for safe TPN administration and reducing complication risks?
Administering total parenteral nutrition (TPN) safely requires a thorough approach that minimizes risks and encourages positive outcomes. One of the most fundamental steps involves using strict aseptic techniques during all aspects of catheter insertion, maintenance, and handling. This includes proper hand hygiene, wearing sterile gloves, using sterile barriers during line access, and adhering to comprehensive disinfection protocols for the insertion site.
Selecting the appropriate central venous access device is crucial. Common options such as peripherally inserted central catheters (PICCs) or tunneled subclavian and internal jugular lines are preferable to reduce peripheral vein irritation and lower line-related complications. The choice depends on the patient's needs and duration of therapy.
Monitoring plays a pivotal role in early identification and management of potential complications. Regular assessments of vital signs, blood glucose levels, electrolytes, liver function tests, triglyceride levels, and acid-base status are recommended. This systematic monitoring allows clinicians to adjust nutrient formulations promptly and prevent issues such as hyperglycemia, electrolyte imbalances, hepatic dysfunction, and metabolic disturbances like refeeding syndrome.
A multidisciplinary team approach enhances the safety and efficacy of TPN therapy. Collaboration among physicians, dietitians, pharmacists, and nursing staff ensures individualized patient care. This team can tailor the nutrient composition based on ongoing assessments, prevent deficiencies, and address emerging complications efficiently.
Preventive strategies extend beyond monitoring. Strict adherence to catheter care protocols—such as secure site dressing changes, regular line flushing with sterile solutions, and timely removal of unused lines—are essential. Implementing minimal enteral nutrition or trophic feeds when possible can also stimulate gastrointestinal function and reduce cholestasis risk.
By integrating these practices— aseptic technique, careful patient and line management, multidisciplinary collaboration, and strict protocol adherence—healthcare providers can significantly lower the incidence of serious TPN-related complications. These measures contribute to safer nutrition support, better clinical outcomes, and improved patient quality of life.
| Practice Area | Recommended Actions | Purpose |
|---|---|---|
| Aseptic Technique | Hand hygiene, sterile barriers, site disinfection | Reduce infection risk |
| Access Device Selection | Use of PICCs or central lines suited for long-term use | Minimize line complications |
| Monitoring and Adjustment | Daily checks of blood glucose, electrolytes, liver function, triglycerides | Detect and correct imbalances early |
| Multidisciplinary Care | Collaboration among doctors, pharmacists, dietitians, nurses | Individualize therapy and improve safety |
| Catheter Care | Dressing changes, line flushing, prompt line removal when no longer needed | Prevent infections and occlusions |
| Nutritional Strategies | Proper formulation, avoid overfeeding, consider cyclic PN | Prevent hepatic and metabolic issues |
This holistic approach aligns with current clinical standards and has been proven effective in reducing the risks associated with TPN, leading to safer patient care and better long-term health outcomes.
Summary and Importance of Vigilant TPN Management
Managing the complications associated with TPN requires a comprehensive approach involving meticulous planning, regular monitoring, and prompt intervention. Understanding the potential risks—metabolic disturbances, infections, hepatic and bone complications, and mechanical issues—and implementing strict preventive measures can significantly reduce adverse outcomes. Collaboration across multidisciplinary teams ensures individualized patient care, early detection of complications, and effective management strategies, ultimately improving safety and efficacy in TPN therapy. Continued vigilance and adherence to best practices are essential for minimizing harms and ensuring optimal patient recovery.
References
- Complications and Monitoring – Guidelines on Parenteral Nutrition ...
- Total Parenteral Nutrition (TPN) Complications
- Total Parenteral Nutrition - StatPearls - NCBI Bookshelf
- TPN Complications and How to Manage Them
- Complication Management - BAPEN
- Parenteral Nutrition: What it Is, Uses & Types - Cleveland Clinic
- Home parenteral nutrition - Mayo Clinic
- Parenteral Nutrition (PN) - Nutritional Disorders - Merck Manuals
- Parenteral Nutrition Risks, Complications, and Management
- Prevention of complications for hospitalized patients receiving ...