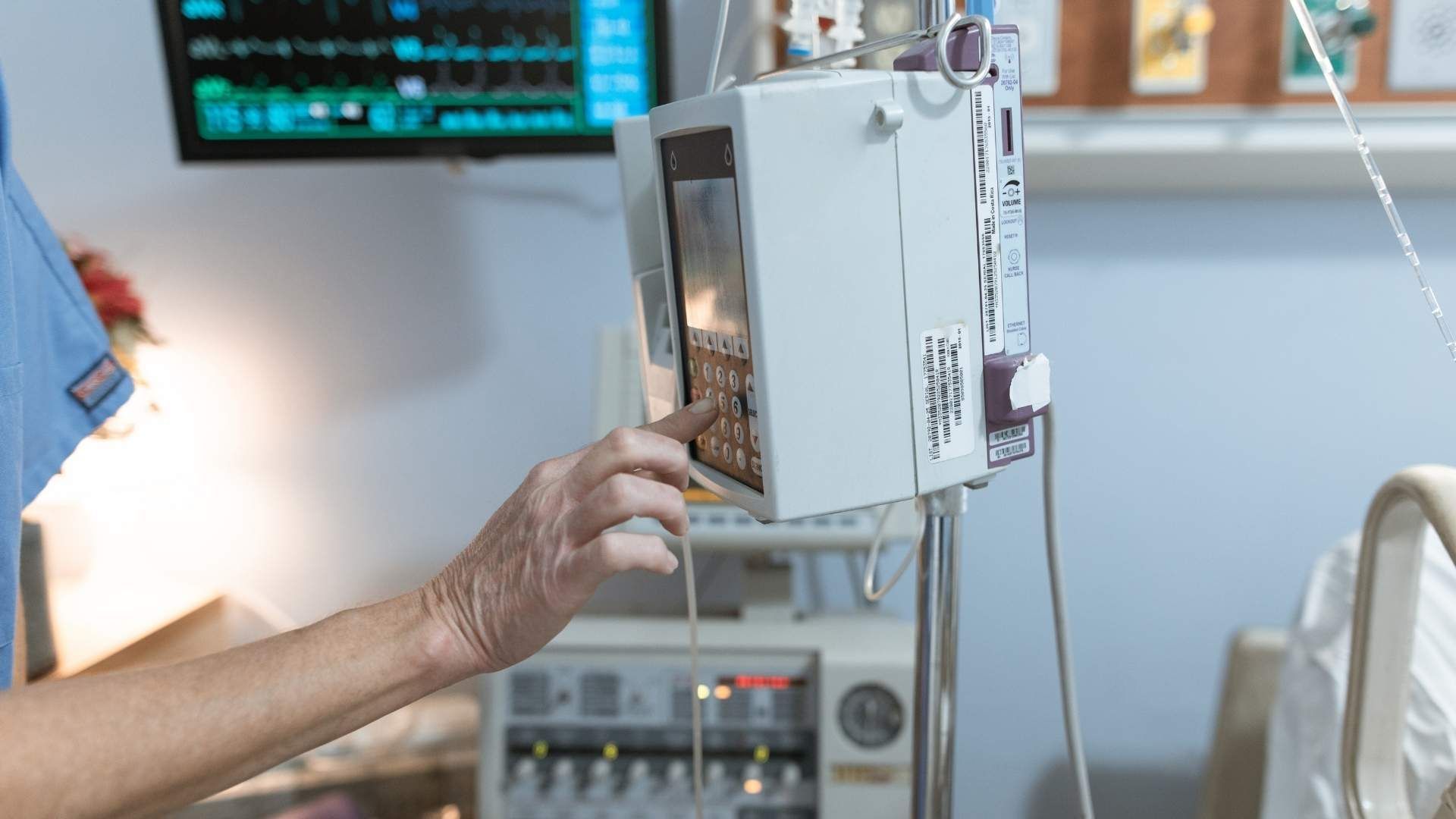
 Parenteral nutrition (PN), particularly total parenteral nutrition (TPN), plays a crucial role in managing patients with inflammatory bowel disease (IBD) who face severe nutritional challenges. It is mainly indicated when oral or enteral nutrition cannot meet patient needs due to complications such as bowel obstructions, high-output fistulas, or intolerance to enteral feeding.
Parenteral nutrition (PN), particularly total parenteral nutrition (TPN), plays a crucial role in managing patients with inflammatory bowel disease (IBD) who face severe nutritional challenges. It is mainly indicated when oral or enteral nutrition cannot meet patient needs due to complications such as bowel obstructions, high-output fistulas, or intolerance to enteral feeding.
 Professional guidelines and research support the strategic use of nutritional therapies, including parenteral nutrition (PN), in managing inflammatory bowel disease (IBD). The European Society for Clinical Nutrition and Metabolism (ESPEN) provides specific indications for PN, emphasizing its role in cases where enteral nutrition (EN) cannot meet nutritional needs, such as with intestinal obstructions, fistulas, or severe malnutrition.
Professional guidelines and research support the strategic use of nutritional therapies, including parenteral nutrition (PN), in managing inflammatory bowel disease (IBD). The European Society for Clinical Nutrition and Metabolism (ESPEN) provides specific indications for PN, emphasizing its role in cases where enteral nutrition (EN) cannot meet nutritional needs, such as with intestinal obstructions, fistulas, or severe malnutrition.
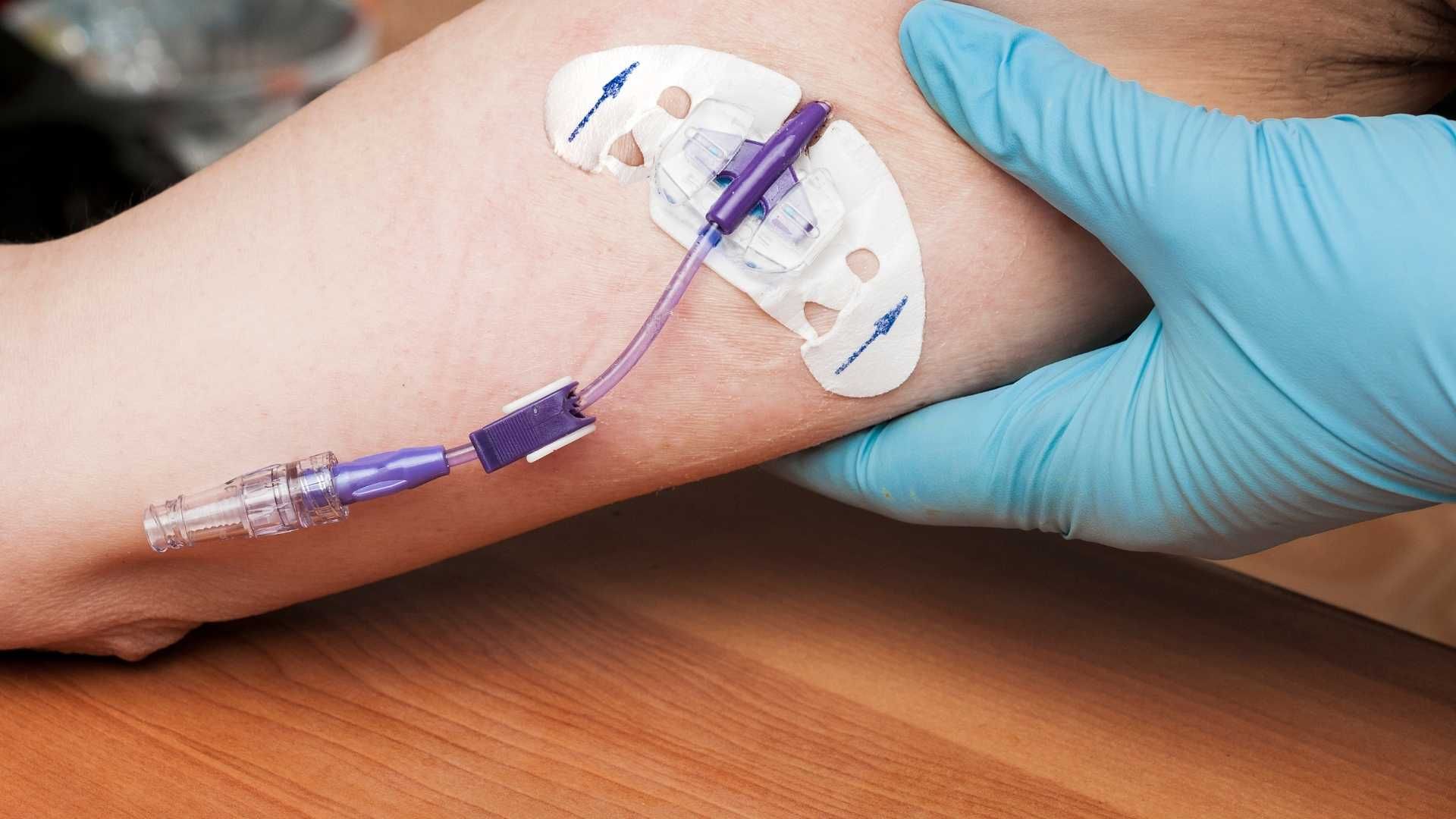
 Parenteral nutrition (PN) is a valuable treatment option for certain patients with inflammatory bowel disease (IBD), but it carries specific risks that require careful management. The most significant complications include infections, particularly bloodstream infections or sepsis related to central venous catheters. Thrombosis of the catheter or associated vessels can also occur, posing additional risks.
Parenteral nutrition (PN) is a valuable treatment option for certain patients with inflammatory bowel disease (IBD), but it carries specific risks that require careful management. The most significant complications include infections, particularly bloodstream infections or sepsis related to central venous catheters. Thrombosis of the catheter or associated vessels can also occur, posing additional risks.