The Role of TPN in Critical Care and Long-Term Nutrition
Understanding TPN: A Cornerstone of Critical Care Nutrition
Total Parenteral Nutrition (TPN) plays a vital role in managing patients who cannot meet their nutritional needs through the gastrointestinal (GI) tract. It involves the intravenous delivery of essential nutrients, supporting recovery and maintaining metabolic functions in critically ill and long-term patients. As medical technology and clinical guidelines evolve, TPN remains an indispensable tool, especially when enteral nutrition is contraindicated or inadequate.
What is Total Parenteral Nutrition (TPN) and How is it Administered?

What is Total Parenteral Nutrition (TPN) and how is it administered?
Total Parenteral Nutrition (TPN) is a medical technique used to deliver essential nutrients directly into a patient’s bloodstream through an intravenous (IV) line. It is typically employed when the gastrointestinal (GI) tract cannot be used effectively due to illness, surgery, or other conditions.
The procedure involves infusing a carefully prepared mixture of nutrients that include carbohydrates, proteins (amino acids), fats (lipids), vitamins, minerals, electrolytes, and fluids. This nutrient solution is designed to meet the specific dietary needs of each patient, ensuring proper metabolic function and supporting recovery.
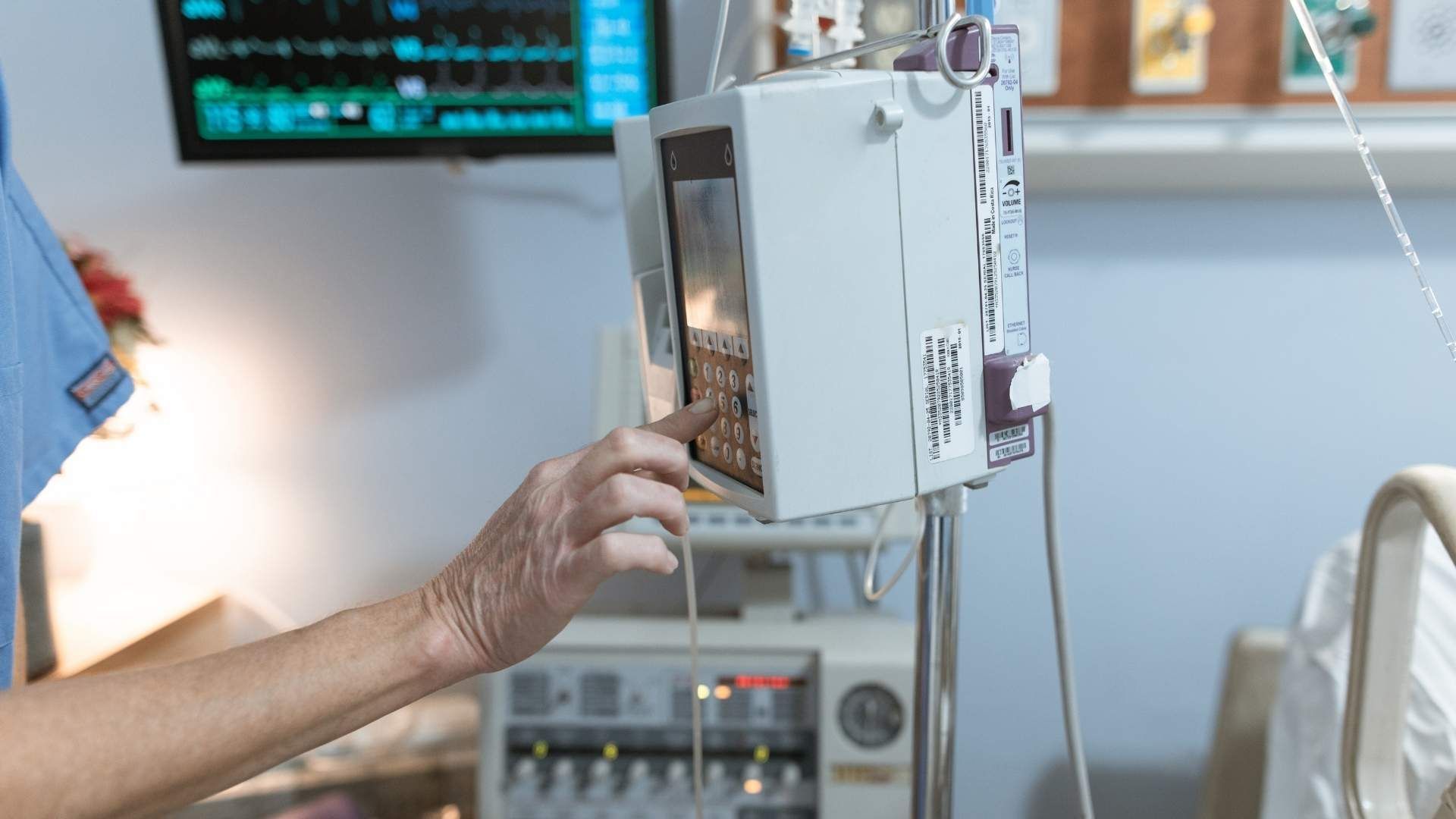
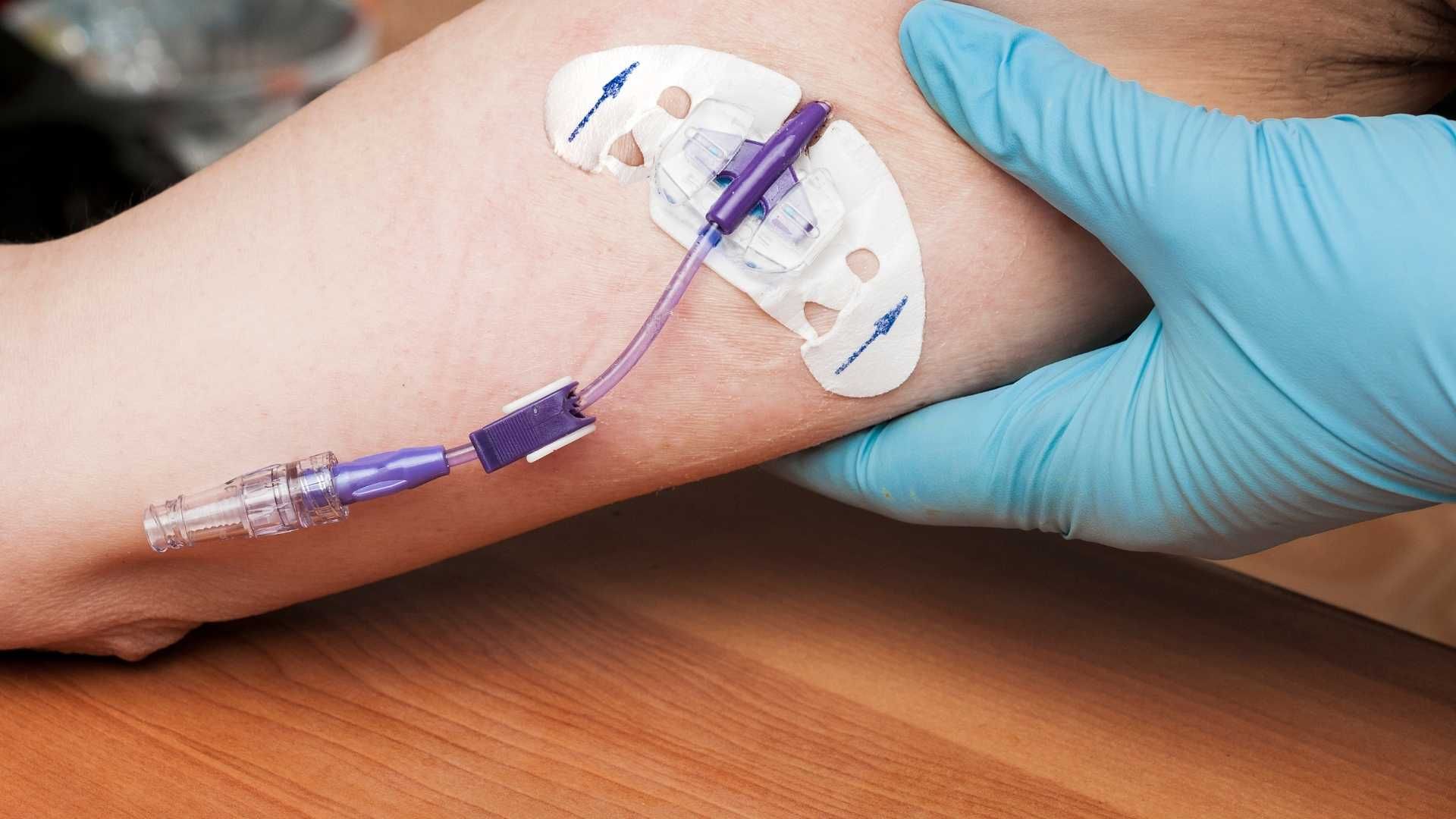
To administer TPN, healthcare professionals insert a central venous catheter—often a surgically placed line into a large vein such as the superior vena cava. This central line allows the high-concentration nutrient solution to be delivered safely and efficiently over an extended period, sometimes days to weeks.
The management of TPN is complex and requires meticulous oversight by specialized healthcare teams. They monitor glucose levels, electrolyte balance, liver function, and overall patient response. Proper line care is crucial to prevent infections, especially catheter-related bloodstream infections, which are a significant complication associated with TPN.
By tailoring the nutrient composition and closely supervising the infusion, TPN provides a vital nutritional option for critically ill patients who cannot tolerate enteral feeding, helping to maintain their metabolic stability during recovery.
The Critical Role of TPN in Acute and Long-Term Nutrition Support
What is the role of TPN in critical care and long-term nutritional support?
Total parenteral nutrition (TPN) plays a vital role in both acute and prolonged clinical scenarios when patients are unable to meet their nutritional needs via the gastrointestinal (GI) tract. It involves delivering essential nutrients directly into the bloodstream through central venous access, bypassing the impaired or inaccessible gut.
In critical care, TPN is often initiated when enteral nutrition (EN) is contraindicated or insufficient, such as in cases of severe gastrointestinal dysfunction, malabsorption, or major gut surgeries. It provides necessary amino acids, carbohydrates, lipids, vitamins, and minerals, tailored to the individual’s requirements.
Long-term, TPN becomes indispensable for patients with persistent gut failure, severe malnutrition, or conditions like gastrointestinal anomalies. It helps maintain nutritional status, supports immune function, and prevents catabolic loss of lean body mass, which is crucial for recovery and overall health.
While TPN can maintain survival and nutritional adequacy, its use must be carefully managed to avoid complications such as metabolic disturbances, infections, and liver complications. Accurate patient assessment, continuous monitoring, and personalized formulations are essential to optimize outcomes.
The development of advanced lipid emulsions, safety protocols, and precise nutritional monitoring have made TPN a safer intervention. Nonetheless, the decision to initiate TPN depends on a comprehensive evaluation of patient needs, potential benefits, and risks.
Support for patients with GI tract failure
For patients whose GI tract cannot fulfill their nutritional requirements, TPN provides a reliable source of nutrition. It ensures the delivery of calories and nutrients necessary for tissue repair, immune competence, and overall recovery, especially in cases of bowel failure, severe trauma, or extensive surgeries.
Management of malnutrition
In critically ill or chronically ill individuals, TPN helps reverse malnutrition, preserve muscle mass, and improve functional status. It is especially important when oral or enteral routes are not sufficient or feasible, preventing deterioration of health and decreasing long-term complications.
Prevention of nutritional deficits
Timely initiation of TPN can prevent deficits in essential nutrients that could impair healing, immune response, and organ function. When early EN is not possible, TPN ensures continuous, adequate nutrition supply, reducing risks of infections, organ failure, and mortality.
| Aspect | Details | Notes |
|---|---|---|
| Indications | GI failure, malabsorption, post-surgical states | When gut cannot be used or tolerated |
| Benefits | Maintains nutrition, supports recovery | Essential in long-term dependence |
| Risks | Infection, liver disease, metabolic disturbances | Requires careful monitoring |
| Monitoring | Blood glucose, electrolytes, triglycerides | Ensures safety and effectiveness |
The effective use of TPN in critical and long-term care hinges on personalized protocols, careful patient selection, and vigilant monitoring to maximize benefits and minimize drawbacks.
Benefits of TPN in Critically Ill Patients

What are the benefits of using TPN for critically ill patients?
Total parenteral nutrition (TPN) plays a vital role in the management of patients who cannot meet their nutritional needs through the gastrointestinal (GI) tract. When enteral nutrition (EN) is contraindicated or insufficient, TPN provides a reliable means of delivering essential nutrients directly into the bloodstream.
One of the primary advantages of TPN is the prevention of malnutrition. Critically ill patients often experience rapid loss of lean body mass due to increased proteolysis and metabolic stress. TPN can help maintain adequate protein and caloric intake, supporting cellular function and organ integrity. Proper nutritional support, especially when tailored to patient-specific requirements and managed by specialized nutrition teams, reduces the risk of complications associated with underfeeding, such as immune suppression, delayed wound healing, and increased morbidity.
Furthermore, TPN supports immune function. Adequate nutrient delivery strengthens immune responses, reducing the incidence of infections and sepsis. In addition, TPN promotes wound healing, critical for patients recovering from surgery or trauma. The provision of amino acids, lipids, and micronutrients like zinc and selenium accelerates tissue repair and regeneration.
Early initiation of TPN in critically ill patients has been linked to positive outcomes such as lower mortality rates, improved caloric and protein intake, and quicker recovery trajectories. Initiating TPN within 24 to 72 hours when enteral feeding is not feasible can prevent energy deficits and related complications.
In summary, TPN ensures critical nutritional support, supports immune defenses, facilitates wound repair, and can lead to better clinical outcomes when used appropriately. Its benefits emphasize the importance of personalized nutrition strategies guided by clinical assessment and monitoring.
| Benefits | Description | Additional Notes |
|---|---|---|
| Prevention of malnutrition | Maintains necessary nutrient levels during critical illness | Especially when EN is contraindicated or insufficient |
| Supports immune function | Enhances pathogen defenses and reduces infection risk | Requires proper micronutrient supplementation |
| Promotes wound healing | Provides building blocks for tissue repair | Critical for post-surgical or trauma recovery |
| Early initiation benefits | Lower mortality and improved outcomes when started early | Typically within 24-72 hours if EN is not feasible |
This tailored approach, with careful monitoring of clinical and laboratory parameters, maximizes the safety and efficacy of TPN in critical care settings.
Risks and Safety Considerations in TPN Administration
What are the risks and complications associated with TPN?
Total parenteral nutrition (TPN) is a lifesaving intervention in critically ill patients who cannot use their gastrointestinal tract. However, it carries a range of potential risks that necessitate careful management and close monitoring.
One of the primary concerns is infectious risk. Central venous access, essential for TPN delivery, can serve as a portal for bloodstream infections such as sepsis. These infections are often related to catheter contamination or improper line care. Catheter-related thrombosis and vascular injury can also occur during line insertion or through long-term use, which may compromise limb or organ function if not promptly addressed.
Metabolic disturbances are common in patients receiving TPN. Hyperglycemia is particularly concerning in ICU settings, requiring tight glucose control to prevent complications. Electrolyte imbalances such as hypokalemia, hypophosphatemia, and hypomagnesemia can occur and need regular assessment. Refeeding syndrome, characterized by shifts in electrolytes, fluids, and metabolic derangements, can be life-threatening if nutrition support is initiated too rapidly.
Hypertriglyceridemia can result from lipid infusion and contributes to pancreatitis and other metabolic issues. Long-term TPN use may lead to liver complications, including fatty liver, cholestasis, and fibrosis, which can compromise liver function and necessitate adjustments in nutrition formulas or discontinuation.
Further, TPN has been linked to metabolic bone disease, such as osteoporosis or osteomalacia, due to nutrient imbalances or deficiencies. Gallbladder stasis and dysfunction can also develop, increasing the risk for gallstones and cholecystitis.
Given these risks, TPN should be administered by an interprofessional team experienced in critical care nutrition. Continuous monitoring of blood glucose, electrolytes, triglycerides, and liver function tests is vital. Proper aseptic technique during line insertion and maintenance, along with protocols for infection prevention, are essential components of safe TPN administration.
Overall, while TPN remains a critical intervention for certain patients, its associated risks underscore the importance of individualized therapy, rigorous monitoring, and adherence to safety protocols to minimize complications and optimize outcomes.
Protocols and Guidelines for Safe TPN Implementation
What guidelines are available for the safe administration of TPN?
The safe administration of Total Parenteral Nutrition (TPN) requires strict adherence to established clinical protocols and guidelines. These protocols serve as a foundation for ensuring patient safety, reducing complications, and optimizing nutritional outcomes.
Firstly, aseptic techniques during the preparation and insertion of central venous catheters are crucial. Proper hand hygiene, sterilization of materials, and the use of full barrier precautions during insertion help prevent catheter-related bloodstream infections, which are common infectious complications.
Monitoring is another essential aspect. Continuous assessment of blood glucose is vital because hyperglycemia can occur if glucose levels are not properly controlled. Regular laboratory tests—including electrolyte panels, liver function tests, and triglyceride levels—are necessary to detect and manage metabolic disturbances early.
Nutritional assessment plays a critical role in planning TPN therapy. A tailored approach involves calculating individualized caloric and nutrient needs, preferably using indirect calorimetry when available. Nutritional plans should undergo regular review and adjustment by a multidisciplinary team comprising physicians, dietitians, and nurses.
Line insertion and care protocols focus on maintaining line patency and preventing infection. Proper placement verification—via imaging—and routine line care, including disinfection of entry sites, are mandated practices.
Training healthcare staff in recognizing early signs of complications, such as infection, thrombosis, or metabolic imbalance, is vital. This preparedness ensures prompt intervention, minimizing adverse outcomes.
In summary, guidelines for safe TPN management encompass aseptic procedures, vigilant monitoring, personalized nutrition planning, and meticulous line care, all supported by a well-trained clinical team. Following these practices significantly reduces risks and enhances recovery in critically ill patients.
Impact of TPN on Patient Outcomes in Critical Settings
Parenteral nutrition (TPN) plays a vital role in managing critically ill patients, especially when enteral feeding is not possible. Its influence on patient outcomes spans several areas including nutritional status, immune function, and recovery trajectory.
Adequate nutritional support via TPN helps maintain lean body mass and supports immune responses, which are often compromised during critical illness. Proper management of TPN involves individualized formulations based on patient needs, careful monitoring of blood glucose, electrolytes, and triglycerides, as well as infection prevention through sterile techniques and proper line management.
Studies indicate that when appropriately used, TPN can reduce infection rates and accelerate recovery. Early initiation, ideally within 24 to 48 hours of ICU admission, is associated with better energy and protein delivery, leading to improved wound healing and immune function. For instance, research involving 437 patients showed a survival rate of 58% over an average of 1.5 years post-TPN initiation, highlighting its potential benefit.
However, TPN use is not without risks. Overfeeding can lead to complications like hyperglycemia, hypertriglyceridemia, and liver dysfunction. Therefore, strict adherence to protocols, thoughtful patient selection, and ongoing monitoring are crucial to mitigate these risks.
Despite its benefits, TPN is generally considered a rescue nutritional strategy. When enteral nutrition is contraindicated or insufficient, TPN becomes essential for preventing worsening malnutrition and supporting recovery.
In conclusion, with rigorous safety and monitoring measures, TPN can significantly improve outcomes for critically ill patients, supporting quick recovery, reducing infectious complications, and enhancing overall survival rates.
Comparison of TPN with Enteral Nutrition
How does TPN compare to enteral nutrition?
Current clinical guidelines and research evidence suggest that enteral nutrition (EN) is generally preferred over total parenteral nutrition (TPN) when the gastrointestinal (GI) tract is functional and accessible. Enteral nutrition uses the gut for nutrient delivery, supporting the maintenance of gut integrity and immune function. It stimulates the production of immune proteins like secretory immunoglobulin A, which helps prevent bacterial attachment to the intestinal wall, thereby reducing the risk of systemic infections.
In contrast, TPN involves delivering nutrients directly into the bloodstream via a central venous catheter, bypassing the GI tract. While TPN can be lifesaving when enteral feeding is contraindicated, it has higher associated risks, particularly infections related to catheter use. Many infectious complications are more related to the use of invasive lines rather than the nutrition method itself.
Clinical outcomes favor enteral nutrition in many situations. Patients on EN tend to have lower infection rates, shorter ICU stays, and better overall recovery. EN also preserves gut function, aiding in early recovery and reducing the risk of complications such as bacterial translocation and systemic inflammation.
However, TPN remains essential when the GI tract is nonfunctional, inaccessible, or when nutritional goals cannot be met adequately via enteral routes. It provides a vital nutritional bridge in cases like intestinal failure, bowel obstruction, or severe malabsorption.
In summary, whenever feasible, enteral nutrition is preferred due to its physiological benefits and safety profile. TPN is reserved for specific clinical situations where the gut cannot be used for feeding. Properly managed, TPN can be delivered safely, but it carries a higher risk profile than enteral feeding.
Emerging Developments and Future Directions in TPN Practice
What are the current practices, recent developments, and future directions in TPN use?
Total parenteral nutrition (TPN) plays a vital role in managing patients with intestinal failure or when enteral nutrition is not feasible. Currently, TPN is tailored to each patient's specific needs, with protocols emphasizing careful formulation, safety, and monitoring.
Recent progress in TPN includes significant technological advancements. The introduction of sophisticated computer algorithms, artificial intelligence, and electronic health records has enabled clinicians to optimize TPN formulations more accurately. These innovations help in predicting patient requirements, reducing errors, and personalizing therapy.
Lipid emulsions, a key component of TPN, have seen improvements targeting stability and safety. Special lipid sources containing omega-3 fatty acids are now used to modulate inflammation and lower the risk of liver complications.
In response to global shortages and supply chain issues, multimodal strategies such as multi-chamber bags have been developed. These systems combine various nutrients into a single, ready-to-use solution, reducing contamination risk and streamlining administration.
Safety protocols are continually evolving. The adoption of standardized procedures, such as strict line insertion and care bundles, minimizes catheter-related infections and mechanical complications. Monitoring practices now include real-time blood glucose control, liver function tests, and assessment of nitrogen balance.
Looking ahead, the field is moving towards greater personalization of TPN. Using advanced tools like indirect calorimetry, clinicians can more precisely determine energy expenditures, avoiding over- or underfeeding. Customized formulations for vulnerable groups, including preterm infants and patients with complex co-morbidities, are a major focus.
Automation plays an increasing role, with pilot programs exploring the potential of robotic compounding and closed-system delivery to reduce errors and enhance safety.
Research trends highlight the development of novel lipid carriers, immune-modulating nutrients such as arginine and glutamine, and strategies to minimize long-term complications like liver disease. Additionally, clinical trials aim to define optimal timing and dosing, especially in critically ill populations.
Overall, future directions in TPN emphasize safety, personalization, technological integration, and expanding evidence-based practices to improve patient outcomes.
Considerations for TPN in Diverse Patient Populations
Total parenteral nutrition (TPN) is a vital intervention in critical care, especially when enteral nutrition is not feasible. However, its application must be carefully tailored to meet the specific needs of diverse patient groups.
One of the first considerations is age. Pediatric patients, particularly neonates and infants, require precise adjustments in nutrient composition, including amino acids, lipids, and micronutrients, to support growth and development. Conversely, elderly patients may have altered metabolic capabilities or comorbidities such as renal or hepatic impairment, which influence nutrient dosing and monitoring protocols.
Organ failure considerations are also critical. Patients with kidney or liver failure need customized TPN formulations to avoid exacerbating existing issues—such as electrolyte imbalances, acid-base disturbances, or hepatic steatosis. For example, patients with renal failure may require modified amino acid solutions and electrolytes, while those with liver dysfunction may need reduced lipid doses to prevent liver overload.
Metabolic management encompasses careful control of glucose and electrolytes. Hyperglycemia is common in critically ill patients receiving TPN and must be managed through insulin therapy and close blood sugar monitoring. Electrolyte imbalances, including sodium, potassium, and magnesium, require frequent assessment and correction, especially in patients with compromised renal or hepatic function.
Contraindications for TPN include a functional gastrointestinal (GI) tract where enteral feeding is possible and effective. Initiating TPN unnecessarily in such cases increases risks of infection, liver complications, and metabolic disturbances without benefits. Additionally, short-term indications may not warrant TPN, emphasizing that the therapy should be reserved for patients with clear, prolonged GI tract dysfunction or malabsorption.
In summary, the safe and effective use of TPN relies on evaluating patient-specific factors such as age, organ function, and metabolic status. Personalized formulation and vigilant monitoring are essential for optimizing outcomes in different patient populations.
Integration of TPN into Comprehensive Critical Care Protocols
How does TPN fit into overall critical care management?
Total Parenteral Nutrition (TPN) plays a crucial role in managing critically ill patients, especially when enteral nutrition (EN) is not feasible or sufficient. It provides essential nutrients directly into the bloodstream, bypassing the gastrointestinal tract, and is used as an alternative when gut function is compromised.
TPN supports the body's metabolic needs, helps maintain nitrogen balance, and assists in managing the stress response typical of critical illness. It is particularly valuable in cases involving gastrointestinal anomalies, severe trauma, malabsorption, or high-catabolic states where the gut cannot be relied upon for nutrition.
Protocols for TPN emphasize personalized composition, tailored to each patient's requirements, organ failure status, and co-morbidities. Proper formulation includes a careful balance of amino acids, carbohydrates, lipids, electrolytes, vitamins, and minerals.
A critical aspect of TPN management involves transitioning strategies—gradually tapering off TPN as enteral feeding becomes tolerated or established. This transition aims to optimize gut integrity, reduce complications like infections or liver dysfunction, and promote recovery.
Monitoring is paramount. Frequent assessment of blood glucose levels, electrolyte balance, triglyceride levels, and liver function guides adjustments. Use of infusion pumps with strict aseptic techniques and proper line placement minimizes risks.
Post-ICU recovery strategies often include higher-calorie and higher-protein regimens to support neurorecovery and organ rebuilding. These are customized based on ongoing assessment and outcomes.
Integration of TPN into comprehensive care also involves a multidisciplinary team—dietitians, physicians, nurses, and pharmacists—working together to optimize nutrition while reducing potential complications. Adherence to current guidelines ensures safe administration and effective nutrition support.
In summary, TPN is a vital component of critical care nutrition, especially in complex cases where oral or enteral routes are unavailable. Its proper use, alongside monitoring and transition protocols, enhances patient recovery and long-term health outcomes.
Role of Micronutrients and Immunonutrition in TPN
What micronutrients and immunonutrients are essential in TPN?
In total parenteral nutrition (TPN), adding essential micronutrients and immunonutrients is critical for supporting immune functions and reducing inflammation in critically ill patients. Micronutrients such as multivitamins, zinc, selenium, and high doses of vitamin C and D are integral parts of TPN formulations. These elements serve vital roles, including bolstering antioxidant defenses, promoting cellular repair, and supporting metabolic functions.
Immunonutrients like omega-3 fatty acids, nucleotides, and glutamine are included to modulate immune responses effectively. Omega-3 fatty acids, in particular, possess anti-inflammatory properties, which help reduce cytokine storms and inflammatory tissue damage, a common concern in conditions like COVID-19.
Properly tailored supplementation according to the patient's phase of illness and specific needs can mitigate immune suppression and oxidative stress, thus facilitating recovery and decreasing the risk of infections and other complications. Ensuring the optimal inclusion of these nutrients in TPN is a vital aspect of comprehensive critical care, aiming to enhance immune resilience and promote healing in vulnerable and long-term critically ill populations.
Application of TPN in Pediatric Critical Care
How is TPN used in pediatric critical care?
Total parenteral nutrition (TPN) is a vital intervention in pediatric critical care when the gastrointestinal tract cannot be used effectively. It involves delivering essential nutrients directly into the bloodstream, bypassing the gut, which is often compromised during critical illnesses or certain conditions.
In children, TPN supports growth, development, and recovery, especially when enteral nutrition (EN) is insufficient or contraindicated. Because children have higher metabolic rates and specific nutritional needs relative to their size, the formulations are carefully adjusted for calorie density, amino acid concentrations, and micronutrient content.
The use of TPN in pediatric patients spans all phases of illness:
- Acute phase: Focuses on preventing malnutrition and supporting immune function while avoiding overfeeding.
- Stable phase: Aims at maintaining adequate growth and supporting the metabolic recovery process.
- Recovery phase: Supports catch-up growth and neurodevelopment, often requiring higher caloric and protein intake.
Throughout these stages, the goal is to prevent nutrient deficits that can impair organ development, immune responses, and brain growth.
Growth considerations
Growth is a fundamental aspect of pediatric nutrition. TPN formulations must be tailored to support normal growth patterns, which is especially challenging during illness when metabolic demands fluctuate. Evidence suggests that early high doses of amino acids and calories, particularly in the initial days, can sometimes hinder recovery and may negatively impact long-term growth.
Proper management involves gradually increasing caloric and protein intake to meet the child's needs without causing metabolic disturbances such as hyperglycemia or liver issues. Clinical monitoring of growth parameters, body composition, and laboratory markers helps ensure optimal support.
Nutritional phases in children
The nutritional strategy via TPN must adapt to different phases of illness:
- Initial phase: Use lower caloric and protein doses to minimize metabolic stress.
- Mid-phase: Gradually increase targets based on tolerance and clinical status.
- Recovery phase: Aim for full nutritional goals, promoting tissue repair and growth.
It is critical to balance providing enough nutrients for growth and avoiding complications associated with overfeeding, such as fatty liver or metabolic disturbances.
Long-term impacts
Long-term effects of early nutritional support in children remain an important focus of ongoing research. Early high-protein, high-energy TPN has the potential to influence neurocognitive development, organ growth, and metabolic health.
Some studies indicate that aggressive nutritional support during critical illness can improve outcomes, but excessive or poorly monitored feeding may have adverse effects, including liver dysfunction and altered body composition.
Regular assessment and individualized adjustments are essential to optimize outcomes. Future research aims to better define the optimal timing, composition, and duration of TPN in pediatric patients, particularly concerning long-term neurodevelopment and metabolic health.
Micronutrient and Trace Element Management in TPN
How are micronutrients managed in TPN?
In total parenteral nutrition (TPN), ensuring the right balance of micronutrients and trace elements is crucial for supporting immune function, wound healing, and overall recovery. Since critically ill patients often experience altered micronutrient levels due to inflammation and metabolic shifts, careful supplementation and monitoring become essential.
Micronutrient management involves providing adequate vitamins, minerals, and trace elements such as zinc, selenium, and electrolytes. These nutrients are included in standardized or tailored TPN formulations depending on the patient's specific needs, clinical condition, and ongoing laboratory results.
Because inflammation can affect micronutrient distribution and utilization, routine assessment of micronutrient status is challenging. Still, clinicians strive to prevent deficiencies that could impair recovery, while avoiding excesses that might lead to toxicity. For example, zinc plays a vital role in immune response, and selenium acts as an antioxidant, helping to reduce oxidative stress.
Tailored dosing strategies are employed, often guided by clinical judgment and available laboratory data, to optimize immune support and tissue repair. Furthermore, micronutrient supplementation must be adjusted over time, especially in long-term parenteral nutrition, to match the patient's evolving needs during different phases of illness.
Overall, effective micronutrient management in TPN helps enhance recovery outcomes, reduce infection risks, and promote healing, especially in patients with prolonged nutritional support requirements.
Conclusion and Future Perspectives in TPN Therapy
What are the current practices, recent developments, and future directions in TPN use?
Current practices in total parenteral nutrition (TPN) are becoming increasingly personalized, aided by technological advancements such as artificial intelligence and electronic health records. These tools help clinicians customize formulations to meet individual patient needs more precisely, thus optimizing outcomes.
Recent developments focus on enhancing the safety and stability of TPN solutions. Innovations include the creation of lipid emulsions enriched with omega-3 fatty acids, which can modulate immune responses and reduce inflammation. Additionally, there has been an emphasis on ensuring drug compatibility within TPN admixtures and addressing the global shortages of key nutrients through the use of multimodal strategies, such as multi-chamber bags and alternative nutrient sources.
Significant progress has been made in standardizing protocols to minimize delivery errors and improve monitoring practices. The use of advanced safety protocols helps prevent common complications like infections, metabolic disturbances, and liver dysfunction.
Looking ahead, future directions aim to further individualize nutrition therapy through automation, automation-enhanced decision-making, and multidisciplinary approaches involving dietitians, pharmacists, and intensivists. Efforts are underway to refine lipid emulsions and amino acid formulations for vulnerable populations, including preterm and low birth weight infants.
Overall, ongoing research and updates in clinical guidelines seek to enhance the safety, effectiveness, and accessibility of TPN. The integration of innovative technologies and renewed focus on personalized care promises improved long-term outcomes for critically ill and chronically ill patients alike.
Optimizing Outcomes with TPN in Critical Care and Beyond
The effective use of Total Parenteral Nutrition is fundamental in managing patients with complex nutritional needs, particularly in critical care and long-term settings. Proper administration, vigilant safety measures, and personalized formulations are essential to maximize benefits and minimize risks. As research advances, future innovations promise enhanced safety, efficacy, and individualized care, ensuring TPN remains a vital component of comprehensive clinical nutrition. Implementing best practices and multidisciplinary coordination will continue to improve patient outcomes, supporting recovery, survival, and quality of life.
References
- Management of parenteral nutrition in critically ill patients - PMC
- Nutritional Intervention in Critical Care | Respiratory Therapy
- Limited long-term survival after in-hospital intestinal failure requiring ...
- Nutrition considerations for patients with persistent critical illness: A ...
- Development and current use of parenteral nutrition in critical care
- Role of Total Parenteral Nutrition (TPN) in Critically Ill ICU Patient ...
- Nutrition in the intensive care unit: from the acute phase to beyond
- [PDF] Critical Care Nutrition Practice Management Guidelines
- Nutrition therapy and critical illness: practical guidance for the ICU ...