 Total parenteral nutrition (TPN) is a vital intervention for critically ill patients who cannot meet their nutritional needs through enteral feeding. Proper dosing and administration of TPN are essential to maximize benefits and minimize risks.
Total parenteral nutrition (TPN) is a vital intervention for critically ill patients who cannot meet their nutritional needs through enteral feeding. Proper dosing and administration of TPN are essential to maximize benefits and minimize risks.
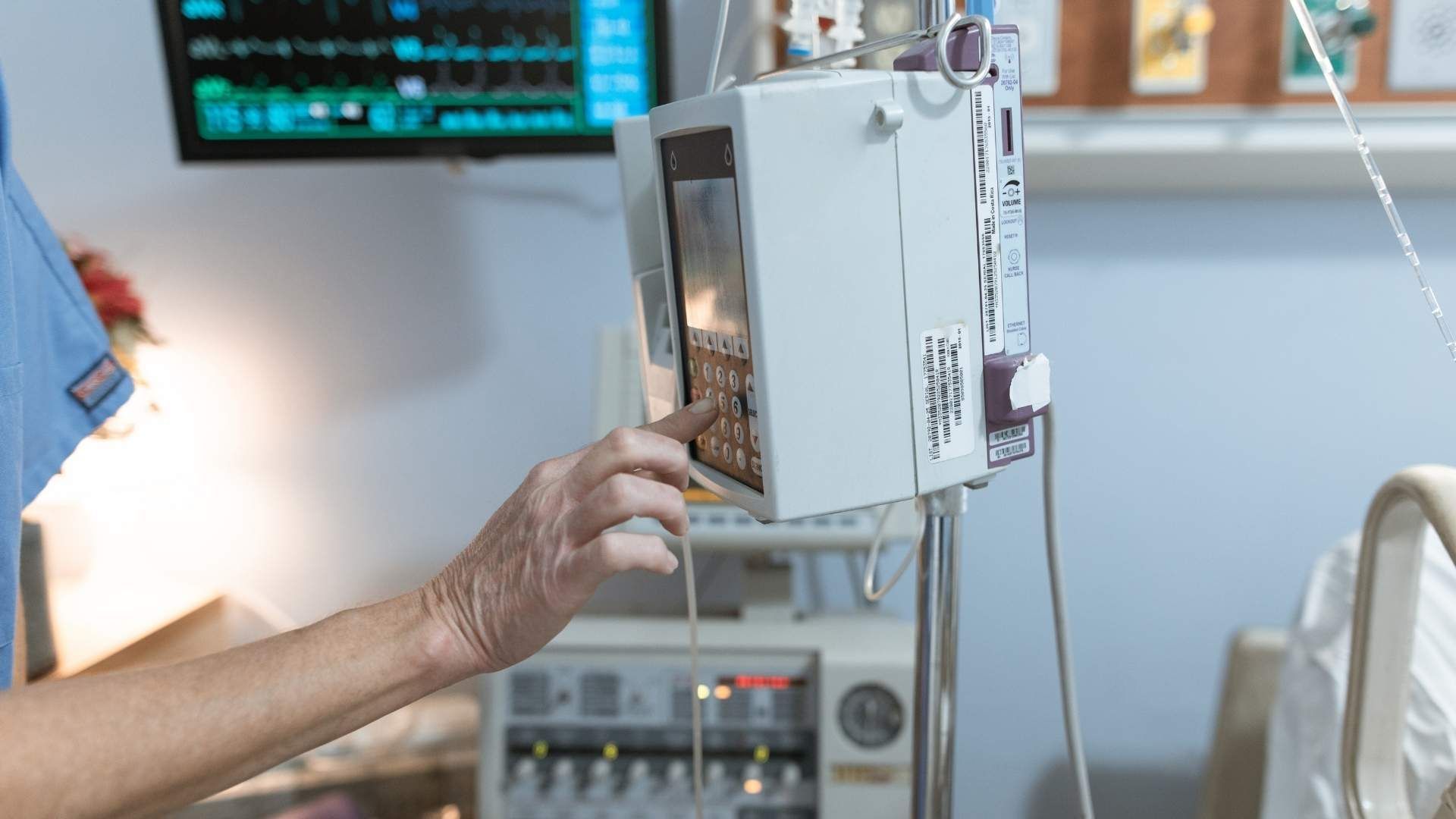
 Parenteral nutrition, particularly total parenteral nutrition (TPN), is an essential aspect of supporting critically ill patients who are unable to receive adequate nutrition through the gastrointestinal (GI) tract. Such situations include gastrointestinal obstructions, extensive bowel resections, or severe fistulae with high output. In these cases, TPN provides a vital supply of nutrients, including amino acids, carbohydrates (dextrose), lipids, vitamins, and minerals.
Parenteral nutrition, particularly total parenteral nutrition (TPN), is an essential aspect of supporting critically ill patients who are unable to receive adequate nutrition through the gastrointestinal (GI) tract. Such situations include gastrointestinal obstructions, extensive bowel resections, or severe fistulae with high output. In these cases, TPN provides a vital supply of nutrients, including amino acids, carbohydrates (dextrose), lipids, vitamins, and minerals.
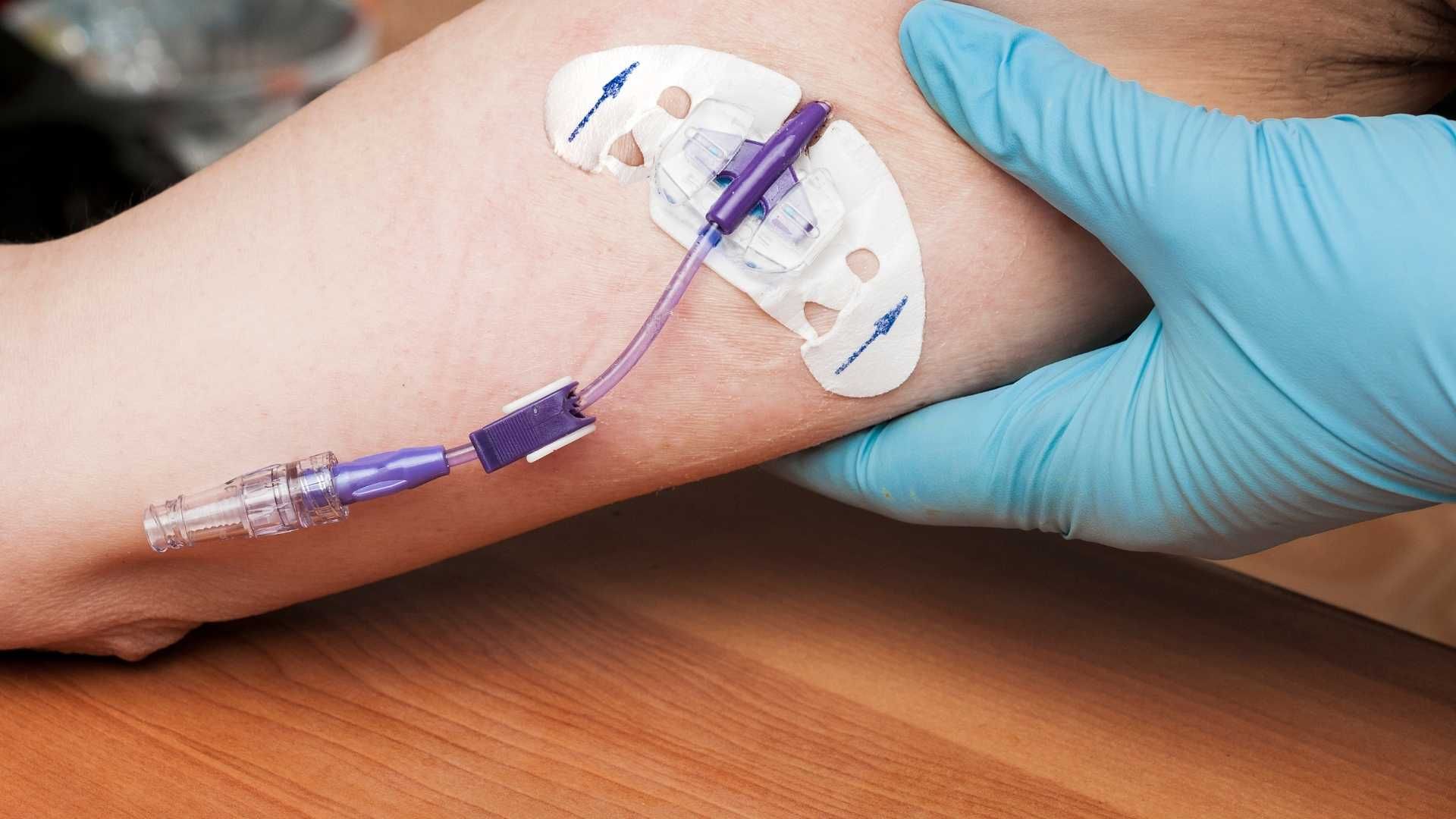
 Total parenteral nutrition (TPN) is a valuable nutritional intervention for critically ill patients who cannot tolerate enteral feeding. However, it is not without risks. One of the most common concerns is metabolic abnormalities. Patients receiving TPN may experience fluctuations in blood glucose levels, leading to hyperglycemia or hypoglycemia. Electrolyte imbalances such as hypokalemia, hypophosphatemia, and hypomagnesemia can also occur, which may cause muscle weakness, arrhythmias, or neurological issues.
Total parenteral nutrition (TPN) is a valuable nutritional intervention for critically ill patients who cannot tolerate enteral feeding. However, it is not without risks. One of the most common concerns is metabolic abnormalities. Patients receiving TPN may experience fluctuations in blood glucose levels, leading to hyperglycemia or hypoglycemia. Electrolyte imbalances such as hypokalemia, hypophosphatemia, and hypomagnesemia can also occur, which may cause muscle weakness, arrhythmias, or neurological issues.
 Overfeeding via total parenteral nutrition (TPN) in critically ill patients can have serious metabolic impacts. One of the primary issues is hyperglycemia, which results from excessive carbohydrate infusion, leading to increased insulin requirements and potential diabetic-like complications. Similarly, high levels of triglycerides due to fat overload can cause hypertriglyceridemia, increasing the risk of pancreatitis and systemic inflammatory responses.
Overfeeding via total parenteral nutrition (TPN) in critically ill patients can have serious metabolic impacts. One of the primary issues is hyperglycemia, which results from excessive carbohydrate infusion, leading to increased insulin requirements and potential diabetic-like complications. Similarly, high levels of triglycerides due to fat overload can cause hypertriglyceridemia, increasing the risk of pancreatitis and systemic inflammatory responses.