TPN for Trauma Patients: Supporting Recovery and Nutritional Healing
Understanding the Critical Role of TPN in Trauma Care
Trauma patients often experience profound metabolic and physiological disturbances that significantly impair recovery. Proper nutritional support, including Total Parenteral Nutrition (TPN), has emerged as a crucial component in optimizing healing, reducing complications, and improving patient outcomes. This comprehensive review explores the principles, practices, and evidence-based strategies surrounding TPN use in trauma management, emphasizing its importance when enteral nutrition is infeasible or insufficient.
The Physiological Foundations of TPN in Trauma Care
What physiological principles underpin the use of TPN in critical trauma conditions?
Total parenteral nutrition (TPN) plays a vital role in the management of critically injured trauma patients by addressing their complex metabolic disturbances. It is founded on fundamental physiological principles aimed at supporting the body's needs when enteral nutrition is not feasible.
Trauma induces a hypermetabolic state characterized by increased energy and protein demands. This response results from hormonal changes, including elevated catecholamines, cortisol, and inflammatory cytokines, which promote catabolism of muscle and lean tissues to supply energy and substrates for healing and immune function. In this state, the body's need for nutrients such as amino acids, glucose, and lipids is amplified.
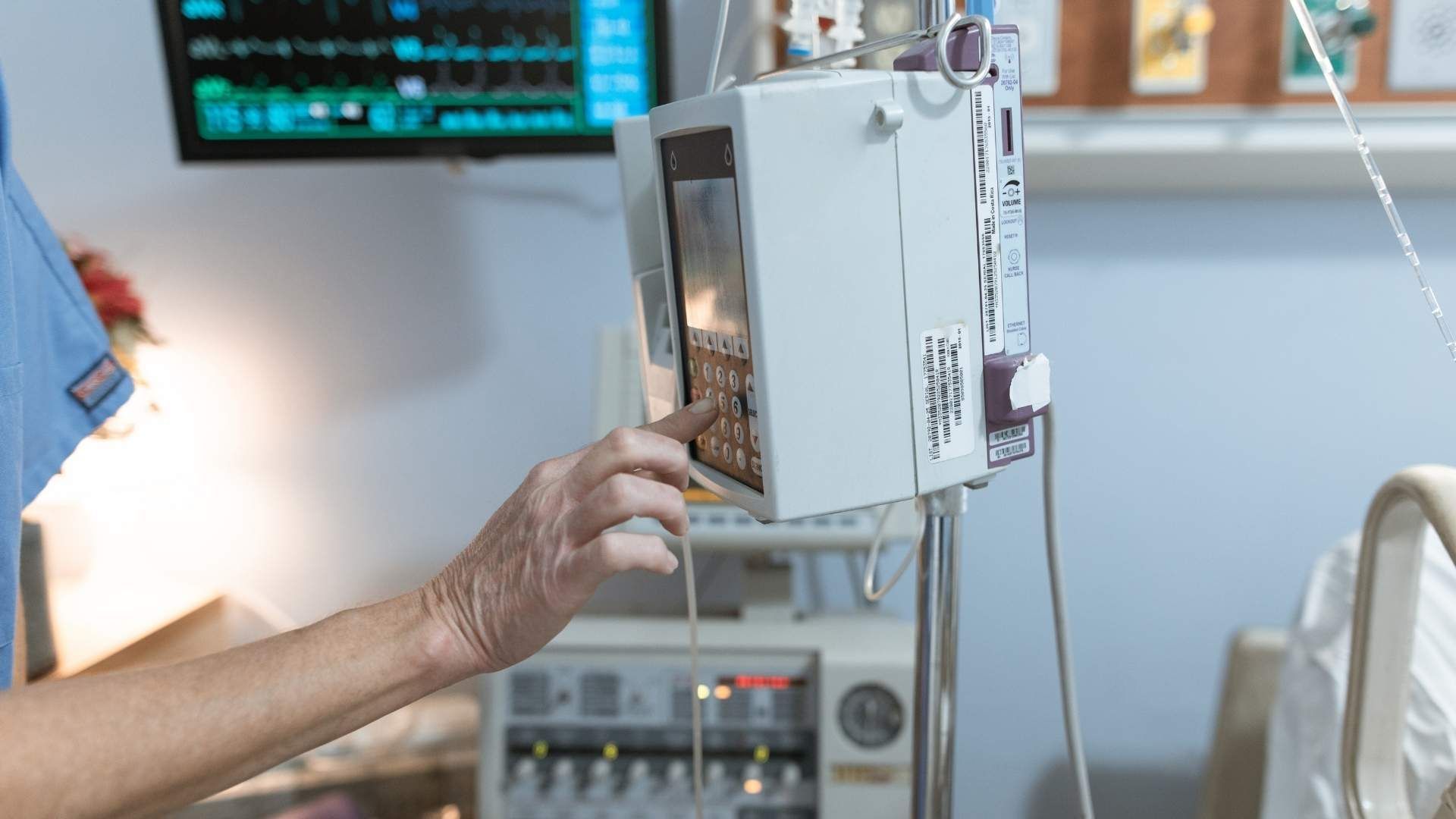
TPN supplies these essential nutrients directly into the bloodstream through central venous access, effectively bypassing a compromised gastrointestinal tract. This is especially critical in conditions like bowel injury, obstruction, or severe diarrhea, where enteral feeding may be contraindicated or impossible.
By delivering caloric and nutritional substrates intravenously, TPN helps meet the increased demands for tissue repair, immune response, and organ function. It ensures that vital processes such as wound healing, infection resistance, and cellular regeneration are maintained. Additionally, TPN assists in modulating metabolic responses such as hyperglycemia and electrolyte shifts, preventing secondary complications.
The physiological mechanism of TPN involves meticulous control of nutrient infusion rates tailored to the patient’s organ function, injury severity, and metabolic state. Careful monitoring of blood glucose, electrolytes, and metabolic parameters helps prevent complications like hyperglycemia, electrolyte imbalances, and infections.
In summary, TPN's physiological foundation lies in its ability to supply complete, balanced nutritional support when the gut cannot be used effectively. It sustains critical metabolic functions, promotes immune competence, and prevents the negative effects of trauma-induced hypercatabolism, ultimately facilitating tissue repair and recovery.
Essential Nutrients for Wound Healing and Recovery in TPN
Why is nutritional healing important in critically injured or trauma patients?
Nutritional healing plays a pivotal role in the recovery of critically injured trauma patients. It provides the foundation for tissue repair, helps strengthen the immune system, and reduces the risk of complications such as infections and delayed wound healing. Adequate intake of calories and high-quality proteins, especially those rich in leucine, supports muscle preservation and repair while counteracting muscle wasting often seen in immobilized, critically ill patients.
In addition to macronutrients, specific micronutrients like vitamins and minerals are essential for immune function and tissue repair. Vitamins such as C and D boost immune responses and promote collagen synthesis, critical for wound healing. Minerals like zinc and selenium are antioxidants that contribute to cellular repair and immune resilience.
Specialized nutrients, including omega-3 fatty acids, have anti-inflammatory properties that help modulate the body's inflammatory response after trauma. These fatty acids can reduce excessive inflammation, which hampers healing, and support cell membrane integrity.
Antioxidants, such as vitamins C and E, combat oxidative stress caused by trauma and inflammation, further aiding the healing process. Together, these nutrients can optimize recovery outcomes by enhancing immune defenses, reducing secondary injuries, and supporting the repair of damaged tissues.
Proper nutritional support, particularly early enteral nutrition that includes immune-modulating formulas, is recommended for trauma patients. These strategies ensure that the body maintains the necessary substrate supply for effective healing, minimizing the risk of malnutrition and promoting faster recovery.
In summary, a comprehensive approach to nutrition that incorporates amino acids, high-quality proteins, vitamins, minerals, and specialized nutrients is crucial for wound healing and recovery in trauma patients. Ensuring these nutrients are part of the nutritional regimen, whether through enteral or parenteral routes, can significantly influence clinical outcomes and long-term health.
Timing and Route of Nutritional Support: When and How to Start TPN
What are the clinical guidelines and best practices for administering TPN in trauma care?
Trauma patients often have complex nutritional needs, and the timing and method of nutritional support are critical for recovery. The current guidelines emphasize that early assessment and individualized nutritional planning are essential. When possible, enteral nutrition (EN) is preferred because it helps maintain gut integrity and immune function.
Initiating EN within the first 24 to 48 hours after the patient becomes hemodynamically stable is generally recommended. The goal is to advance feeding gradually over the next 48 to 72 hours to meet caloric and protein requirements. When enteral feeding alone cannot meet the patient’s needs—such as after 7 to 10 days of therapy with insufficient intake—or in cases where the gastrointestinal (GI) tract cannot be used at all (due to contraindications or high risk), parenteral nutrition (PN) becomes necessary.
PN should then be started promptly to prevent malnutrition and support wound healing. The initiation of TPN should be carefully managed, with close monitoring for complications such as infections, electrolyte imbalance, and refeeding syndrome. Electrolytes should be repleted as needed, and vitamin supplements—particularly B vitamins and vitamin D—are important to prevent deficiencies.
Monitoring practices favor thorough clinical assessment over routine reliance on serum proteins, which are affected by acute phase responses. Assessments include physical examination, evaluation of GI tolerance, and radiographic studies if indicated. Importantly, serum markers like albumin or prealbumin are not reliable for short-term nutritional assessment in critical illness.
Furthermore, GI intolerance should be evaluated clinically, focusing on symptoms like abdominal distension, vomiting, or high gastric residuals, rather than solely relying on residual volume measurements.
Overall, the safe administration of TPN requires a multidisciplinary approach, timely intervention, and vigilant monitoring, ensuring that nutritional needs are met without increasing the risk of complications.
Risks and Complications of TPN in Trauma Patients
What are the risks and contraindications associated with TPN use in trauma patients, and how are they managed?
Total parenteral nutrition (TPN) is an essential tool for supporting trauma patients who cannot meet their nutritional needs enterally. However, its use comes with potential risks and contraindications that require careful management.
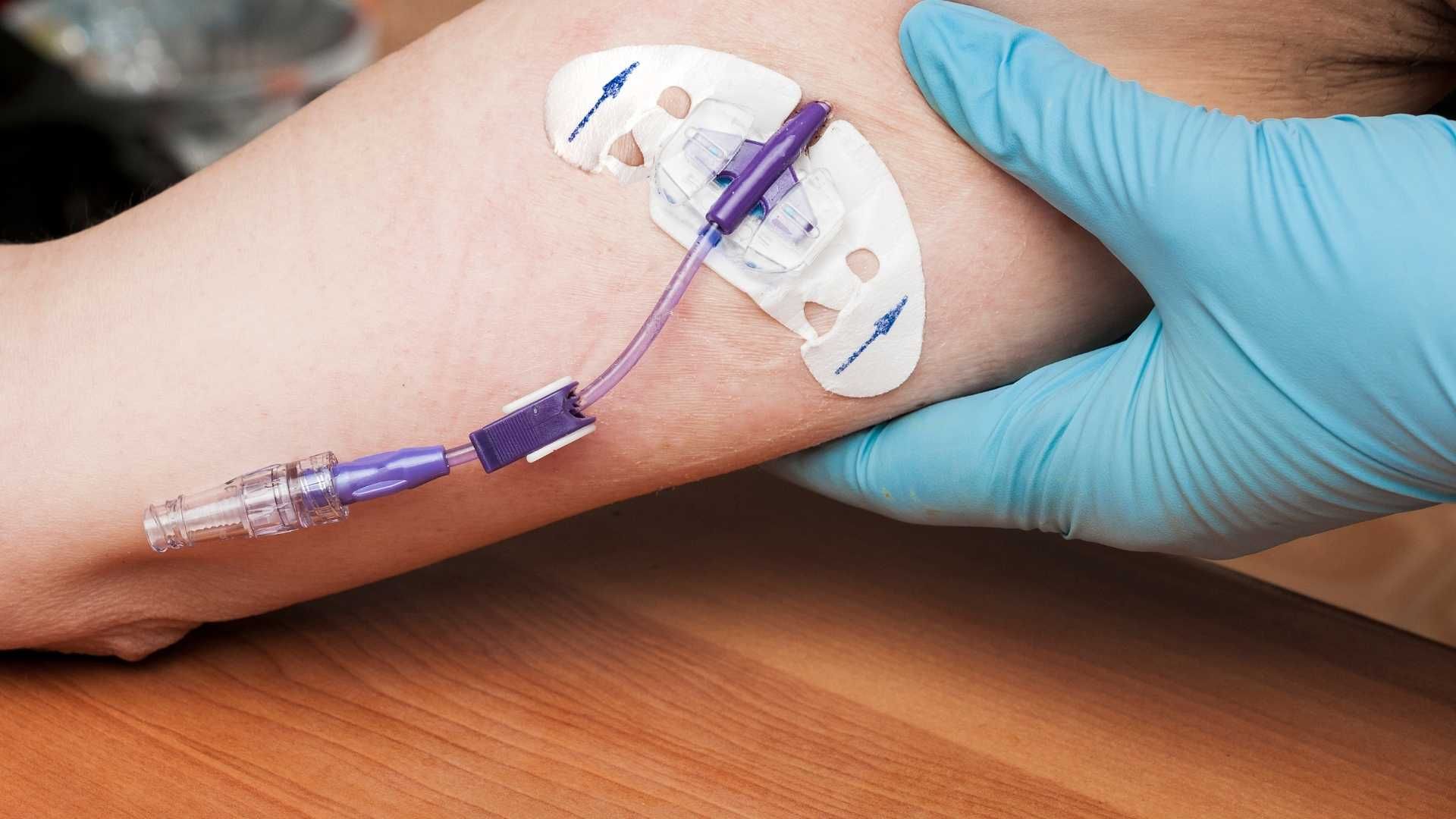
One of the primary concerns is infection risk. Since TPN involves the use of central venous access, there is a significant chance of bloodstream infections, including catheter-related bloodstream infections (CRBSIs). Strict aseptic techniques during catheter insertion and maintenance are vital to minimize this risk. Regular catheter site care, proper hand hygiene, and routine surveillance help prevent infections.
Metabolic abnormalities are common complications. Hyperglycemia is frequently observed due to the high glucose load in TPN solutions. Monitoring blood glucose levels daily allows for timely insulin administration to control hyperglycemia. Refeeding syndrome is another serious concern, especially in malnourished or chronically ill patients. It involves shifts in electrolytes and fluid balance upon initiating nutrition and requires gradual repletion of calories, along with electrolyte and vitamin supplementation, particularly thiamine.
Electrolyte imbalances, such as hypokalemia, hypophosphatemia, and hypomagnesemia, may occur and need correction based on regular blood work. Lipid disturbances can also develop, including hypertriglyceridemia; triglyceride levels should be monitored regularly, and lipid infusion should be adjusted accordingly.
Liver-related complications such as fatty liver and cholestasis can develop from long-term TPN use. Regular assessment of liver function tests is essential, and strategies such as cycling TPN (administering it only during certain hours) and reducing lipid load can mitigate these issues.
Vascular access problems, including pneumothorax, bleeding, thrombosis, and catheter dislodgement, pose additional risks, especially with prolonged catheter use. Proper insertion technique, secure catheter placement, and vigilant monitoring are critical. Use of ultrasound guidance and choosing appropriate catheter type can reduce adverse events.
In summary, while TPN is invaluable in managing critically injured trauma patients, awareness and proactive management of its risks through careful monitoring, aseptic technique, and interdisciplinary collaboration are vital to minimize complications and optimize patient outcomes.
Evidence and Outcomes of TPN in Trauma Care
Total parenteral nutrition (TPN) has long been considered a valuable tool in the management of critically ill trauma patients, especially when enteral nutrition (EN) is not feasible. Emerging evidence suggests that when used appropriately, TPN can support immune function, promote wound healing, and help maintain metabolic stability.
The timing of TPN initiation is critical. Current guidelines recommend starting TPN if a patient cannot meet at least 50% of their caloric needs enterally by day 5 post-injury and if contraindications to EN persist. Early initiation within the first 24-48 hours, particularly in patients with gastrointestinal dysfunction, can help prevent negative energy balance and muscle wasting.
However, recent studies highlight potential risks associated with early and aggressive use of TPN. For instance, early PN in patients who are tolerating EN has been linked to higher rates of bloodstream infections and other nosocomial infections. Therefore, careful patient selection and timing are paramount—delaying TPN until after confirming gut function or when enteral feeding is insufficient has been associated with reduced infection rates.
In terms of recovery and mortality, evidence indicates that tailored TPN regimens—using modern lipid emulsions based on omega-3 fatty acids or olive oil—can decrease infection risks and improve overall outcomes. Incorporating indirect calorimetry to precisely measure energy expenditure allows customized nutrition plans, potentially leading to better wound healing and shorter hospital stays.
In summary, well-managed TPN can be a crucial component of trauma care, providing essential nutrients when enteral feeding is impossible or inadequate. Nonetheless, judicious timing, careful monitoring, and individualized plans are necessary to maximize benefits and minimize complications.
Special Considerations for Trauma Patients with Specific Injuries
How can nutritional interventions, including TPN, support patients with specific injuries such as traumatic brain injury?
Traumatic brain injury (TBI) creates a complex metabolic state characterized by hypermetabolism and hypercatabolism. This high level of metabolic activity significantly increases the body’s energy and nutrient requirements, which if unmet, can lead to muscle wasting, immune suppression, and poorer neurological outcomes.
Early nutritional support is critical. Initiating enteral nutrition (EN) within 24 to 48 hours after injury helps maintain gut integrity, supports immune function, and may reduce infection risks. For patients with TBI, this approach is especially important as the gut plays a central role in systemic recovery. When enteral feeding is not tolerated or contraindicated, parenteral nutrition (PN) becomes necessary, typically after about a week, to meet the elevated caloric and protein demands.
Protein intake of approximately 1.2 to 2.0 g/kg/day is recommended to support neural repair and prevent muscle loss. Precise caloric needs are best determined via indirect calorimetry, which provides tailored energy expenditure estimates to avoid overfeeding or underfeeding.
Moreover, incorporating neuroprotective nutrients such as omega-3 fatty acids, antioxidants, and micronutrients like vitamins B, C, D, and E may enhance neural regeneration and functional recovery. Although evidence is still evolving, these nutrients have shown promise in supporting brain repair processes.
In summary, individualized nutritional strategies—using both early EN and suited PN when necessary—combined with targeted neuroprotective nutrients, are vital in optimizing outcomes for patients with traumatic brain injury.
Socioeconomic Factors and Disparities in TPN Access
How do insurance and socioeconomic status influence TPN use in trauma care?
Traumatic injury management often includes nutritional support, especially when enteral feeding is not feasible. Parenteral nutrition (PN), particularly total parenteral nutrition (TPN), plays a critical role in supporting wound healing and recovery in severely injured patients. However, evidence shows that socioeconomic factors significantly influence access to this vital therapy.
Research analyzing data from over 2.4 million adult trauma patients indicates that TPN use is relatively rare, with only about 1,831 receiving the intervention. Notably, patients with higher injury severity and penetrating trauma are more likely to be administered TPN. Meanwhile, demographic factors such as age also play a part.
A substantial disparity exists based on insurance coverage. Patients with private insurance and Medicare are significantly more likely to receive TPN than uninsured individuals. Multivariable analysis reveals that increasing age, penetrating injury, and high injury severity scores correlate with higher TPN utilization, but there is a marked decrease in its use among uninsured patients.
What impact does socioeconomic status and insurance coverage have on TPN utilization?
These disparities underline broader issues of resource allocation and healthcare inequities within trauma care systems. Uninsured patients often have less access to advanced nutritional interventions like TPN, which may negatively affect their recovery outcomes. This is especially concerning considering that nutritional support is crucial in managing complex biological responses to trauma, such as hypermetabolism and wound healing requirements.
The variation in TPN administration based on socioeconomic status suggests structural barriers hinder equitable care delivery. Patients without sufficient insurance coverage or those from lower socioeconomic backgrounds might not receive the same level of nutritional support as their insured counterparts, risking poorer recovery trajectories.
How can we address these disparities?
Addressing the inequality in TPN access necessitates systematic policy changes. Hospitals and healthcare systems should aim to standardize protocols ensuring that all trauma patients, regardless of socioeconomic status, have equal access to nutritional evaluation and support.
Policy efforts could include expanding coverage for nutritional therapies, integrating nutrition support as a fundamental component of trauma treatment, and allocating resources to reduce disparities. Hospitals might also develop targeted programs to identify and support underinsured or uninsured patients, such as financial assistance or community-based interventions.
Furthermore, fostering awareness among healthcare providers about disparities can lead to more equitable decision-making processes. Overall, ensuring equitable access to TPN not only improves individual patient outcomes but also advances the goals of fairness and excellence in trauma care.
Integrating Multidisciplinary Teams and Monitoring for Optimal Outcomes

Role of trauma and dietitian teams
Effective nutritional management in trauma patients depends heavily on the coordinated efforts of trauma surgeons, critical care physicians, and dietitians. These multidisciplinary teams collaborate to assess the patient's pre-existing nutritional status, injury severity, and the ability to tolerate enteral or parenteral nutrition.
Dietitians are particularly crucial in planning individualized nutritional support strategies, selecting appropriate formulas (such as high protein, elemental, or specialized formulas), and establishing feeding protocols aimed at early initiation within 24 to 48 hours of admission. They monitor ongoing nutritional needs, adjusting the plan based on the patient’s progress, metabolic demands, and any complications that arise.
Trauma teams focus on stabilizing the patient hemodynamically and ensuring safe access for nutritional routes. Regular communication between teams helps in timely transition from enteral to parenteral nutrition when necessary, especially in cases of gut dysfunction or contraindications.
Monitoring nutritional progress and complications
To optimize recovery, continuous monitoring of nutrition therapy is vital. This includes biweekly weight checks, weekly assessments by trauma dietitians, and daily discussions between PICU and trauma teams to evaluate nutritional adequacy.
Clinical examination remains the cornerstone for detecting complications such as gastrointestinal intolerance, high gastric residuals, diarrhea, or signs of refeeding syndrome like electrolyte imbalances. Routine laboratory tests—metabolic panels, electrolytes, triglycerides, blood glucose—are essential for detecting metabolic disturbances and guiding ongoing nutrition adjustments.
Imaging studies or nutritional bio-markers are used selectively, emphasizing clinical assessment over routine serum proteins, which can be misleading in acute settings.
Protocols for advancing nutrition and preventing refeeding syndrome
Protocols for nutritional support are designed to minimize risks and promote safe advancement. Early feeding often begins with trophic or low-volume feeds, progressing cautiously toward caloric goals.
Special attention is given to prevent refeeding syndrome, which involves metabolic disturbances such as hypophosphatemia, hypokalemia, and hypomagnesemia. To mitigate these risks, electrolyte levels are corrected preemptively, and feeding is gradually increased—typically over 24 to 48 hours—while administering vitamin supplementation particularly thiamine.
The use of indirect calorimetry can help tailor caloric administration accurately, avoiding overfeeding and reducing the risk of complications. For patients with high nutritional risk or significant deficits, supplemental parenteral nutrition is initiated early if enteral routes cannot meet at least 60% of caloric requirements after 7–10 days.
By integrating multidisciplinary efforts with vigilant monitoring and stepwise advancement of nutrition, clinicians can enhance recovery outcomes, reduce complications, and improve survival rates in critically ill trauma patients.
Future Directions and Research in Nutritional Support for Trauma

What evidence exists regarding the benefits, timing, and outcomes of TPN in trauma management?
Recent studies and clinical reviews suggest that total parenteral nutrition (TPN) can be a valuable component of trauma treatment when used appropriately. Evidence indicates that TPN is safe and effective as an alternative route when enteral nutrition is not feasible or insufficient—particularly in cases of severe gastrointestinal dysfunction, high-output fistulas, or after extensive bowel resection.
The timing of TPN initiation remains a subject of ongoing research. While early TPN—started within 24-48 hours—can help offset the hypermetabolic and hypercatabolic response immediately following trauma, some evidence points to potential adverse effects if started prematurely in patients who can tolerate enteral feeds. Delaying TPN until after confirming gut function or when enteral nutrition cannot meet 50% of caloric needs by day 5 may help reduce infectious complications.
Studies have shown that improper use of early TPN, especially when overfeeding occurs, may increase the risk of bloodstream infections and other nosocomial infections. Conversely, targeted application with individualized assessment—guided by indirect calorimetry and careful monitoring—can improve wound healing and immune response.
Advances in lipid formulations, such as omega-3 fatty acid-enriched lipids, have been associated with reduced infection rates and liver dysfunction, further enhancing TPN safety. Moreover, tailored nutrition, including micronutrient supplementation like vitamins and trace elements, plays an important role in optimizing outcomes.
In conclusion, the optimal use of TPN requires a personalized approach. Proper assessment of the patient’s gut function, infection risk, and metabolic status is essential to balance the benefits of supporting recovery with potential risks. When incorporated correctly, TPN remains a vital tool in comprehensive trauma care.
Long-term outcomes and functional recovery
Emerging research emphasizes the importance of early and adequate nutritional support not only during the acute phase but also throughout post-discharge rehabilitation. Proper nutrition influences long-term muscle mass retention, functional status, and quality of life.
Patients who receive targeted nutritional therapy early tend to have better wound healing, fewer infections, and shorter hospital stays. Nonetheless, long-term data on functional recovery underscores the need for ongoing nutritional interventions alongside physical therapy and other rehabilitation strategies.
Further studies are required to evaluate how specific nutrients impact recovery trajectories and to identify optimal timing for transitioning from acute to maintenance nutrition.
Longitudinal studies and clinical trials
There is a significant gap in large-scale, randomized controlled trials assessing long-term functional outcomes after trauma related to different nutritional strategies. Future research should focus on longitudinal studies that track patient recovery over months or years, examining how early intervention influences mobility, cognition, and independence.
These trials should also explore the cumulative effects of micronutrients, dietary patterns, and combined therapies like exercise with nutrition to develop integrated rehabilitation protocols.
Innovations in nutritional formulas and delivery methods
Technological advances are paving the way for more precise nutrition delivery. Novel formulations, including immune-modulating ingredients, specialized amino acid blends, and lipid emulsions, are being tested for their potential to enhance healing and immune function.
Delivery methods are also evolving, with developments in micro- and nano-encapsulation enabling targeted nutrient release and reduced side effects. Use of portable and automated infusion systems could improve patient convenience and adherence, particularly in long-term outpatient settings.
Overall, these innovations aim to personalize and optimize nutritional care, ultimately improving functional outcomes and quality of life for trauma patients.
The Future of Nutritional Care in Trauma Patients
As the understanding of trauma-specific nutritional needs advances, integrating evidence-based strategies like early assessment, individualized TPN protocols, and multidisciplinary collaboration will be crucial. Continued research into long-term outcomes, innovative formulas, and delivery methods will further refine optimal nutrition support, ultimately enhancing recovery, reducing complications, and improving the quality of life for trauma patients. Ensuring equitable access to these advanced nutritional therapies remains a priority for the global health community.
References
- Nutritional Intervention for a Critically Ill Trauma Patient
- The Use of Parenteral Nutrition and Disparities in Its Allocation ...
- Is Total Parenteral Nutrition (TPN) an Evil in Trauma Patients?
- Nutritional support for head‐injured patients - PMC - PubMed Central
- Nutritional support in trauma
- [PDF] NUTRITION SUPPORT OF THE TRAUMATICALLY INJURED ...
- Total parenteral nutrition: potion or poison? - ScienceDirect
- Nutritional Support Following Traumatic Brain Injury
- 42. Nutritional Support Using Enteral and Parenteral Methods - TCCC