TPN in Post-Surgical Patients: Why It’s Needed and How It Helps
Understanding the Critical Role of TPN in Postoperative Care
Total Parenteral Nutrition (TPN) is a vital part of the nutritional management of post-surgical patients who cannot meet their nutritional needs through enteral feeding. By delivering essential nutrients directly into the bloodstream, TPN supports healing, immune response, and overall recovery, particularly in patients with impaired gastrointestinal function or contraindications to enteral nutrition. This article explores the indications, benefits, administration considerations, and risks associated with TPN in surgical settings, emphasizing its importance in optimizing patient outcomes.
What is Total Parenteral Nutrition (TPN) in Surgical Patients and When Is It Indicated?
What is total parenteral nutrition (TPN) in surgical patients and when is it indicated?
Total parenteral nutrition (TPN) is an essential method of delivering all necessary nutrients directly into the bloodstream via intravenous infusion. In surgical patients, TPN becomes especially important when the gastrointestinal (GI) tract cannot be used for feeding due to disease or injury.
In the context of surgery, TPN is primarily indicated for patients with conditions that impair or contraindicate enteral nutrition. These include severe gastrointestinal disruptions such as chronic intestinal obstruction, bowel pseudo-obstruction, high-flow fistulas, or postoperative bowel leaks. It is also crucial for patients with short bowel syndrome, severe malabsorption conditions, or complex fistulas where enteral feeding cannot meet the metabolic needs of the patient.
Patients who are unable to eat or tolerate oral intake for more than a week—particularly in ICU or post-surgical settings—may also benefit from TPN to prevent malnutrition. This method provides complete nutritional support, including lipids, dextrose, amino acids, vitamins, electrolytes, minerals, and trace elements, all carefully customized according to individual requirements.
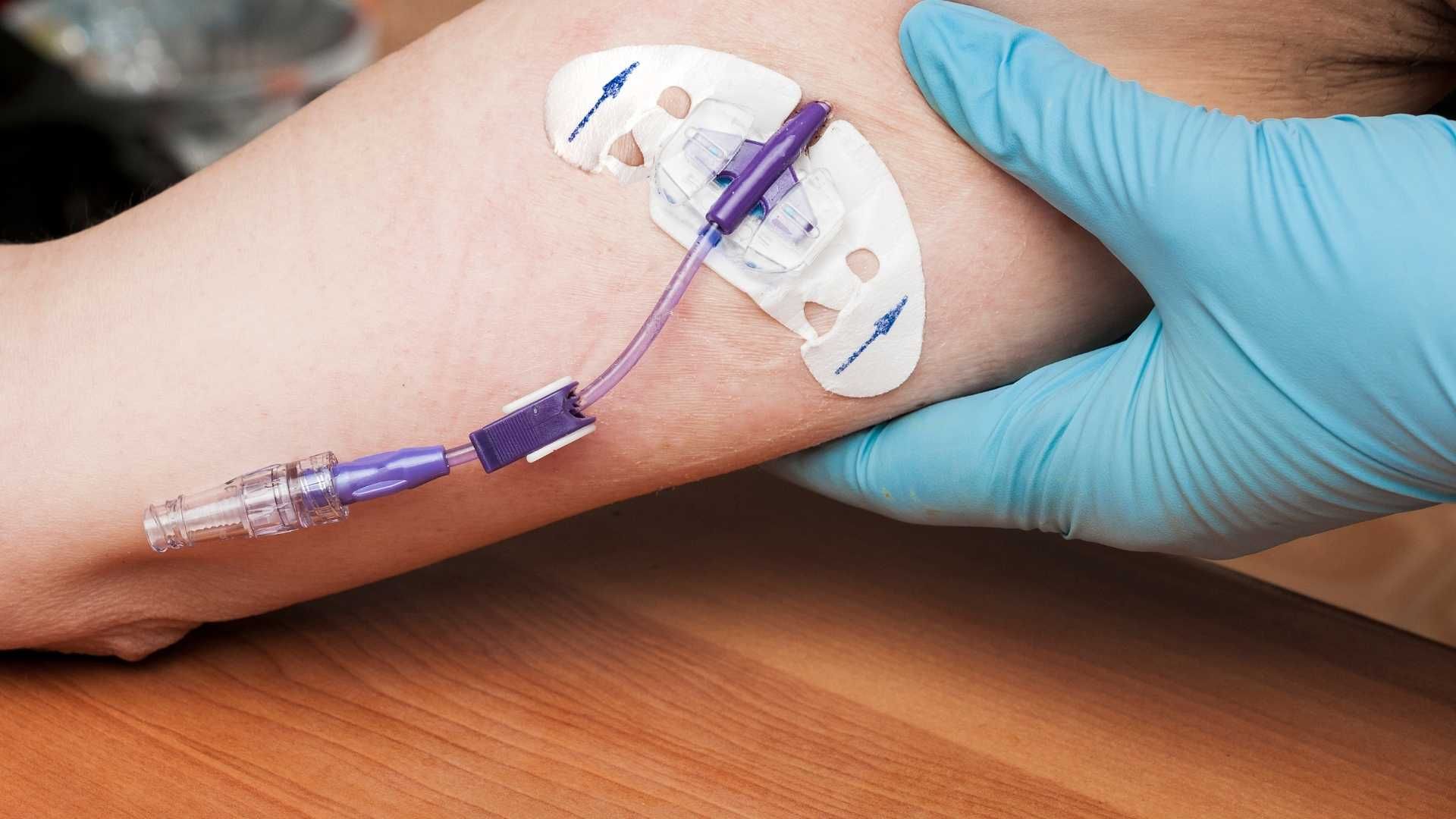
Since TPN solutions are hyperosmolar, they are administered through central venous access devices, such as PICC lines or central venous catheters. These large-bore veins reduce the risk of phlebitis and allow safe infusion of nutrient-rich fluids.
Monitoring is a vital component of TPN therapy. It involves regular checks of blood glucose, electrolytes, liver function tests, and clinical status to detect any complications early. Potential adverse effects include bloodstream infections, metabolic disturbances like hyperglycemia, electrolyte imbalances, and liver dysfunction.
In summary, TPN is a critical intervention for surgical patients with contraindications to enteral feeding, providing lifesaving nutrition until GI function is restored or feeding can be safely resumed.
Clinical Indications for Using TPN Post-Surgery
What are the clinical indications for using TPN after surgery?
Total parenteral nutrition (TPN) is a vital tool in managing surgical patients who cannot meet their nutritional needs through the normal gastrointestinal route. Its primary role is to provide essential nutrients directly into the bloodstream when the digestive system is compromised or unsuitable for feeding.
One of the main scenarios where TPN becomes indispensable is when patients experience severe gastrointestinal dysfunctions such as bowel obstruction, pseudo-obstruction, or bowel leaks. These conditions prevent the normal passage and absorption of nutrients, rendering enteral feeding unsafe or impossible.
Patients with significant malabsorption syndromes, including short bowel syndrome or extensive bowel resection, often rely on TPN for nutritional support. Postoperative complications that impair digestion or absorption, like high-output fistulas, ileus, or bowel ischemia, also necessitate the use of TPN.
In addition, TPN is indicated when patients are expected to be NPO (nothing by mouth) for more than 7 to 10 days. During this period, the body’s nutritional needs must be met to promote healing, immune function, and prevent muscle wasting.
Patients undergoing major trauma or suffering from sepsis often experience hypermetabolic states, increasing their nutritional requirements beyond what can be supplied enterally. TPN helps to meet these heightened metabolic demands.
The decision to initiate TPN involves a multidisciplinary team, including surgeons, dietitians, and physicians, to assess the benefits versus the potential risks. This team considers contraindications, such as the presence of infections or vascular access issues, while ensuring that TPN is used judiciously to optimize patient outcomes.
In summary, TPN post-surgery is clinically indicated when the gastrointestinal tract cannot function effectively to support nutritional needs, especially in cases of severe bowel dysfunction, extended NPO status, or when metabolic demands are increased due to critical illness.
Benefits of TPN in Surgical Patient Recovery

What benefits does TPN provide to surgical patients in recovery?
Total parenteral nutrition (TPN) plays a vital role in the recovery process for surgical patients, especially those who cannot meet their nutritional needs through oral or enteral routes. One of the primary benefits is its ability to help stabilize serum nutrient levels, ensuring that the body receives the essential macronutrients and micronutrients required for healing.
TPN supplies a balanced mixture of lipids, dextrose, amino acids, vitamins, minerals, and trace elements tailored to the patient’s individual needs. This targeted nutritional support promotes optimal wound healing by providing the raw materials necessary for tissue synthesis and repair. Adequate nutrition accelerates the restoration of skin integrity, reduces the risk of wound complications, and shortens hospital stays.
Beyond wound healing, TPN supports immune function, which is crucial in the postoperative period. Malnutrition impairs immune responses, increasing susceptibility to infections. By maintaining adequate nutritional status, TPN enhances the body’s ability to fight infections, thereby reducing postoperative complications.
Moreover, TPN helps prevent metabolic disturbances such as hypoglycemia, electrolyte imbalances, and refeeding syndrome, which can occur if nutritional support is not properly managed. It also reduces the physiological stress of surgery, leading to better overall recovery outcomes.
Research indicates that in severely malnourished patients, preoperative or perioperative TPN can significantly improve clinical results. For instance, it has been associated with decreased noninfectious complications and an improved nutritional state prior to major surgery.
In summary, TPN offers a comprehensive nutritional strategy that stabilizes nutrient levels, accelerates healing, supports immunity, and enhances the overall recovery process for surgical patients who are unable to receive adequate nutrition through other means.
Nutritional stabilization
TPN maintains serum nutrients within optimal ranges, which is essential in the immediate postoperative period when normal intake is compromised.
Wound healing
Providing necessary amino acids and energy sources facilitates tissue repair, collagen synthesis, and wound closure.
Immune support
Adequate nutrition supports immune cells and reduces the risk of infections, a common complication after surgery.
| Aspect | Benefit | Additional Notes |
|---|---|---|
| Nutritional Stabilization | Keeps nutrients and energy levels steady | Prevents hypoglycemia and electrolyte abnormalities |
| Wound Healing | Promotes tissue repair and reduces healing time | Requires adequate protein and micronutrient supply |
| Immune Support | Enhances immune response, reducing infection risk | Important in immunocompromised or severely malnourished patients |
Overall, TPN is a critical intervention that, when appropriately used, can significantly improve surgical recovery, especially in malnourished or high-risk patients.
How TPN Supports Healing and Recovery in Surgical Patients
How does TPN support surgical patients’ healing and recovery?
Total parenteral nutrition (TPN) is a crucial intervention for surgical patients who cannot meet their nutritional needs through oral or enteral routes. When the gastrointestinal (GI) tract is impaired—due to conditions like bowel obstruction, fistulas, or post-surgical bowel rest—TPN provides essential nutrients directly into the bloodstream, ensuring that the body maintains adequate nutritional status.
This method of nutrition significantly improves nitrogen balance, which is vital for tissue repair and wound healing. By supplying a well-balanced mix of amino acids, glucose, lipids, vitamins, and minerals, TPN supports the synthesis of new tissue, accelerates recovery, and reduces the risk of postoperative complications such as infections, delayed wound healing, and organ dysfunction.
Immune function also benefits from TPN. It promotes lymphocyte recovery and enhances immune responses, thus helping the body's defenses against infections common in postoperative patients. Maintaining immune competence is particularly important for severely malnourished patients or those with increased metabolic demands due to trauma or major surgery.
Although enteral nutrition remains the preferred method of support because of its ability to preserve gut integrity and stimulate immune responses, TPN is indispensable when enteral feeding is contraindicated or insufficient. By ensuring a continuous supply of vital nutrients, TPN plays a vital role in optimizing surgical outcomes, improving immune resilience, and supporting faster recovery.
In summary, TPN facilitates tissue repair, sustains immune defenses, and improves overall healing in patients unable to receive adequate nutrition enterally. Its judicious use is essential for managing complex surgical cases and enhancing patient recovery.
Postoperative TPN Administration: Formulation and Management Considerations
What are the considerations for administering TPN postoperatively, including formulation and management?
When administering total parenteral nutrition (TPN) after surgery, it is crucial to carefully customize the nutrient solution to meet the individual needs of each patient. This process involves tailoring the composition, including carbohydrates, amino acids, fats, electrolytes, vitamins, and trace elements, based on the patient’s metabolic requirements and clinical condition.
The formulation must follow established guidelines—such as those from ASPEN—to ensure that the patient receives adequate energy and nutrients without overfeeding, which can cause metabolic complications. For most adult patients, the caloric goal falls between 30 to 35 kcal/kg/day, with roughly 50% to 70% of calories provided by carbohydrates, and 20% to 30% by lipids. The protein intake is typically aimed at 1.5 to 2 g/kg/day, and nitrogen administration should be around 250 to 300 mg/kg/day.
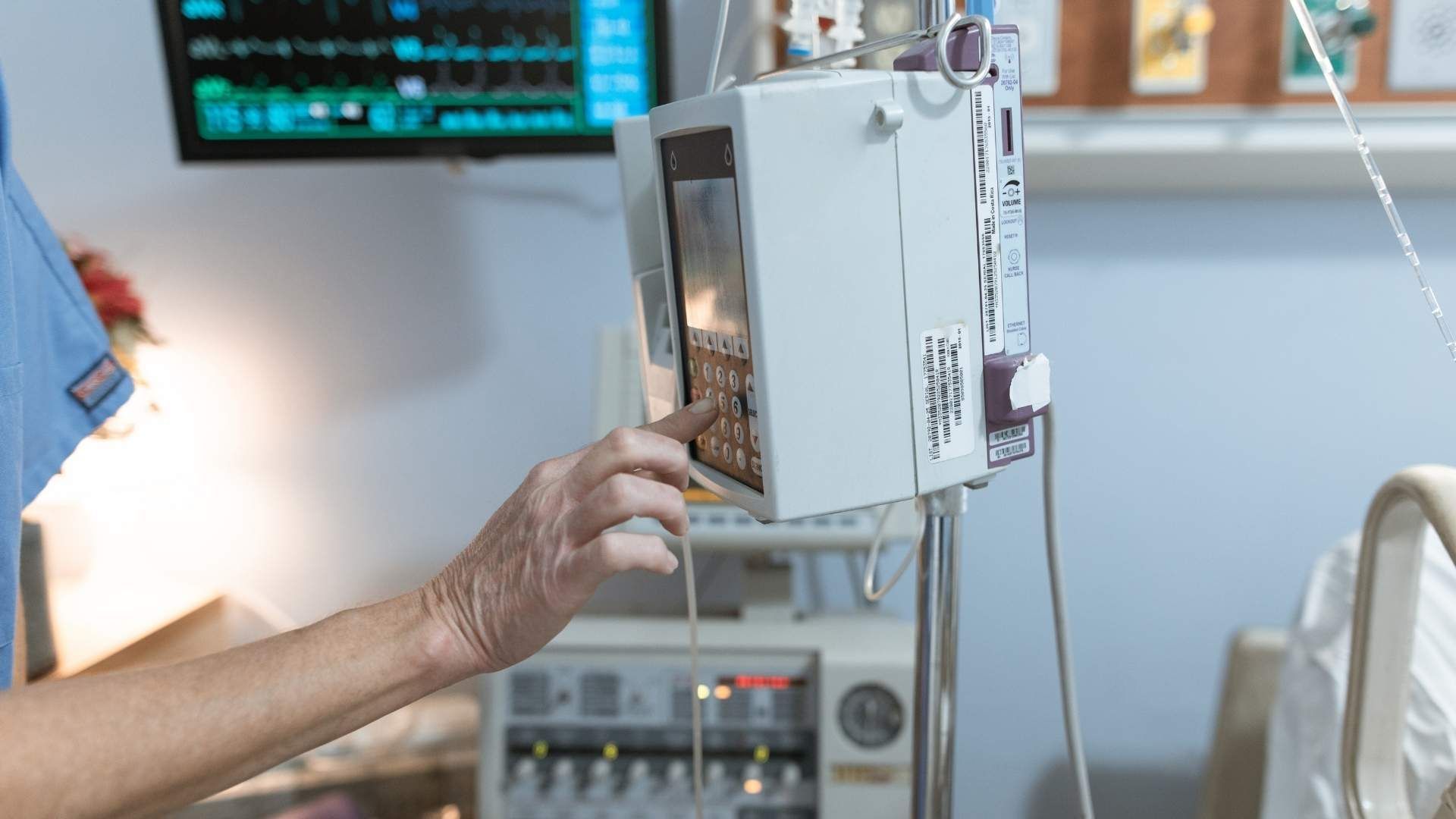
Administration of TPN requires central venous access due to its high osmolarity. Common access points include peripherally inserted central catheters (PICC lines), central venous catheters, or implantable ports. The solution is delivered using an infusion pump to ensure precise control of the delivery rate, usually set to be infused over 10 to 12 hours, often at night to facilitate ease of monitoring during waking hours.
Preparation and verification of TPN involve strict aseptic techniques to prevent contamination. This includes inspecting the solution for particulates and contamination, labeling it correctly, and following protocols for medication additions if necessary. The pharmacy prepares the TPN solution in advance, usually for 24-hour continuous infusion, with the composition confirmed before administration.
Monitoring is a vital component of postoperative TPN management. Healthcare providers should regularly assess the patient’s clinical status, including vital signs, hydration status, and signs of infection at the catheter site. Laboratory tests are performed frequently, especially in the initial days, to monitor electrolytes, blood glucose levels, liver function tests, and signs of metabolic disturbances.
Special attention should be paid to preventing and managing potential complications such as hyperglycemia, hypoglycemia, refeeding syndrome, electrolyte imbalances, catheter-related infections, and thrombosis. Blood glucose levels are often checked every 4-6 hours during the initial phase of TPN therapy, with adjustments made to insulin or TPN composition as needed.
Line care involves aseptic handling to prevent bloodstream infections. Proper disconnection procedures, secure line fixation, and meticulous sterile technique during access or medication changes are critical.
Documenting each step of TPN administration, including infusion rates, patient response, and laboratory results, helps to ensure safety and allows for prompt adjustments.
In summary, postoperative TPN management demands a comprehensive approach that integrates tailored formulation, meticulous administration techniques, diligent patient monitoring, and precise documentation. This ensures that the nutritional support effectively contributes to recovery while minimizing risks of complications.
Risks and Complications of TPN in Surgical Patients
What are the risks and complications associated with TPN in surgical patients?
Total parenteral nutrition (TPN) is a vital intervention for patients unable to meet nutritional needs through oral or enteral routes. However, it is not without potential risks that can impact recovery and overall outcomes.
One of the most significant concerns is infection. TPN requires the placement of central venous access devices such as PICC lines, central venous catheters, or implantable ports. Poor aseptic technique during insertion or maintenance can lead to bloodstream infections, including central line-associated bloodstream infections (CLABSIs), skin infections, and catheter-related sepsis. These infections can prolong hospital stays and increase morbidity.
Metabolic disturbances are common in patients receiving TPN. These include hyperglycemia, which may necessitate insulin adjustments, hypoglycemia upon abrupt discontinuation, and electrolyte imbalances like hyponatremia or hyperkalemia. Refeeding syndrome is a serious concern in malnourished patients, characterized by rapid shifts in electrolytes that can cause cardiac and respiratory complications. Lipid overload can lead to hypertriglyceridemia, while deficiencies in vitamins and minerals may impair healing.
Long-term TPN use can cause liver-related complications. Hepatic steatosis (fatty liver), cholestasis, fibrosis, and in severe cases, cirrhosis are well-documented side effects affecting approximately 15% to 40% of long-term TPN patients. These conditions can impair liver function and complicate management.
Metabolic bone disease is also associated with prolonged TPN, leading to osteoporosis and osteomalacia due to deficiencies of calcium, vitamin D, and other minerals. Vascular and mechanical issues are prevalent, especially with improper catheter placement or handling. Thromboembolism and venous thrombosis can occur, obstructing vessels or dislodging emboli. Mechanical complications like pneumothorax or air embolism may happen during catheter insertion or manipulation, posing life-threatening risks.
Systemic issues such as dehydration or fluid overload can occur if TPN is not carefully balanced, affecting cardiac and pulmonary function. Oxygenator failure in patients on extracorporeal support with TPN might result in hypoxia.
Overall, the importance of meticulous monitoring cannot be overstated. Regular assessment of electrolytes, liver function tests, blood glucose levels, and clinical signs is crucial for early detection and management of these potential complications.
Below is a summary table highlighting these risk categories:
| Risk Category | Typical Complications | Additional Considerations |
|---|---|---|
| Infections | CLABSIs, skin, catheter-related sepsis | Strict aseptic technique is essential |
| Metabolic disturbances | Hyperglycemia, hypoglycemia, electrolyte imbalances, refeeding syndrome | Regular monitoring and gradual initiation |
| Liver complications | Steatosis, cholestasis, fibrosis, cirrhosis | Long-term TPN increases risk |
| Vascular issues | Thrombosis, catheter malposition, pneumothorax, air embolism | Proper insertion and maintenance are crucial |
| Systemic effects | Dehydration, fluid overload, oxygenator failure | Balance fluid and monitor parameters continuously |
Understanding these risks enables healthcare providers to implement preventive measures, ensuring safer TPN administration and better patient outcomes.
Timing of TPN Initiation After Surgery
When should TPN be initiated after surgery?
The appropriate timing for starting total parenteral nutrition (TPN) following surgery hinges on a patient's specific gastrointestinal function and overall nutritional status. In many cases, if a patient cannot tolerate enteral nutrition within 24 to 48 hours after surgery, clinicians consider initiating TPN to fulfill their nutritional requirements.
For patients experiencing impaired gut motility, such as ileus or bowel obstruction, TPN should be started promptly if enteral feeding remains unfeasible or inadequate. Early nutritional intervention can help mitigate complications related to malnutrition, promote healing, and support immune function.
However, the decision to initiate TPN is individualized. It involves assessing factors like the severity and duration of gastrointestinal dysfunction, the patient’s baseline nutritional reserves, and potential risks associated with parenteral nutrition.
While some guidelines advocate for early initiation within 24 hours for severely malnourished or high-risk patients, others recommend delaying until gastrointestinal function shows signs of recovery. Delaying TPN beyond 48 to 72 hours without gastrointestinal support is generally discouraged because prolonged fasting can exacerbate malnutrition.
In summary, early TPN initiation—usually within the first 24 to 48 hours—is appropriate in patients with significant gut impairment or malnutrition, provided that careful monitoring and individualized clinical judgment guide the timing. Conversely, in patients who can tolerate enteral nutrition, this is preferred due to better safety and outcome profiles.
Evidence Supporting the Use of TPN in Surgical Recovery
What is the evidence supporting the effectiveness of TPN in improving postoperative recovery?
Research into total parenteral nutrition (TPN) reveals a nuanced picture of its benefits and limitations in surgical patient recovery. Multiple studies, including randomized controlled trials and meta-analyses, have investigated how TPN influences wound healing, complication rates, and overall survival after major surgeries.
One significant study is the Veterans Affairs TPN Cooperative Study, which examined the effects of preoperative TPN in malnourished surgical patients. The findings showed that TPN improved noninfectious postoperative complications, such as wound infections and delayed healing, especially in severely malnourished individuals. However, the same research indicated an increased incidence of infectious complications like bloodstream infections, suggesting TPN's potential risks when used indiscriminately.
Further meta-analyses have demonstrated that while TPN may not reduce mortality generally, it can significantly decrease the likelihood of major complications, including postoperative wound infections, sepsis, and pulmonary issues, particularly in patients with pre-existing malnutrition.
Importantly, timing and patient selection are crucial. Early initiation of TPN within 24 to 48 hours can benefit critically ill or severely malnourished patients, but delaying TPN for up to a week in well-nourished patients often results in stable recovery and fewer infections.
Collectively, evidence underscores that TPN can support recovery by maintaining or restoring adequate nutritional status, which is essential for wound repair, immune competence, and reducing catabolic stress. Yet, it also emphasizes the importance of cautious, individualized application to avoid potential adverse effects.
Impact on wound healing and complications
Nutritional status critically impacts wound healing, immune defenses, and complication rates after surgery. Malnourished patients frequently experience delayed healing, increased infection risk, and longer hospital stays.
Studies consistently show that TPN administered pre- or postoperatively in malnourished patients enhances wound healing by providing essential amino acids, energy, and micronutrients needed for tissue repair.
Moreover, patients receiving TPN have demonstrated fewer non-infectious complications like fistulas or wound dehiscence when nutritional therapy is properly tailored. Conversely, if TPN is used inappropriately or excessively, there is a risk of complications such as bloodstream infections, liver dysfunction, and metabolic disturbances.
Therefore, while TPN can be a valuable tool to promote wound healing and reduce some postoperative complications, its benefits are maximized when carefully targeted to patients with documented nutritional deficits and used within a well-monitored, multidisciplinary framework.
Below is a summary table comparing different aspects of TPN application in surgical recovery:
| Aspect | Evidence | Outcome | Notes |
|---|---|---|---|
| Timing of initiation | Early (within 48 hours) | Improved recovery in malnourished | Delay may be beneficial in well-nourished |
| Patient selection | Severe malnutrition | Reduced non-infectious complications | Increased infection risk if used indiscriminately |
| Impact on wound healing | Adequate TPN | Better wound repair and fewer infections | Requires individualized nutrient formulation |
| Adverse effects | Excessive use | Elevated infection and metabolic issues | Necessitates strict monitoring |
This evidence collectively emphasizes the importance of individualized, cautious use of TPN in surgical patients to optimize recovery outcomes.
Guidelines and Best Practices for TPN in Postoperative Care

What are the recommended patient selection criteria for postoperative TPN?
Selecting the right patients for postoperative TPN is essential for safe and effective outcomes. TPN is typically indicated when patients cannot meet their nutritional needs through enteral routes for at least 7 days, especially if they have contraindications such as bowel obstruction, fistulas, or severe malnutrition. Particular attention is given to patients with significant malnutrition, as they are more susceptible to postoperative complications and may benefit from preoperative or early postoperative TPN. Accurate assessment involves evaluating clinical status, body weight, laboratory markers like serum albumin, and physical examination.
How should monitoring be carried out during TPN therapy?
Monitoring is vital to avoid and manage potential metabolic complications associated with TPN. Guidelines recommend frequent laboratory tests, including electrolyte panels, liver function tests, blood glucose levels, and triglycerides. Monitoring should be conducted initially every 6 hours during the first 24-48 hours or until metabolic stability is achieved, then gradually extended. Clinicians should observe for signs of refeeding syndrome, hyperglycemia, electrolyte disturbances, cholestasis, and catheter-related infections. Regular clinical assessments, including weight, hydration status, and catheter site inspections, are also part of comprehensive monitoring.
When should TPN be discontinued postoperatively?
Discontinuing TPN requires careful evaluation of the patient's nutritional status and ability to resume enteral or oral intake. Once the patient demonstrates adequate gastrointestinal function and can meet at least 60-70% of their caloric and protein needs through enteral feeding, TPN can be gradually tapered. The guideline suggests stopping TPN when enteral nutrition supplies more than 50% of caloric requirements. In some cases, TPN duration is typically 7-14 days, but it may extend if the patient remains incapable of tolerating enteral feeds. Close assessment of biochemical parameters and clinical progress ensures safe cessation and transition to oral or enteral nutrition.
The Overall Significance of Nutritional Support in Postoperative Outcomes
What is the overall importance of nutritional support, including TPN, in surgical recovery?
Nutritional support is a fundamental aspect of patient recovery after surgery. Proper nutrition, whether enteral or parenteral, helps improve wound healing by providing essential nutrients like proteins, vitamins, and minerals that are vital for tissue repair.
It also strengthens the immune system, reducing the risk of infections—a common complication in postoperative patients. For example, studies have shown that targeted nutritional interventions can lower the incidence of wound infections and sepsis, particularly in malnourished individuals.
While enteral nutrition (EN) is generally preferred due to its safety, cost-effectiveness, and benefits for maintaining gut integrity, there are cases where parenteral nutrition (PN), including total parenteral nutrition (TPN), becomes necessary. TPN is especially critical for patients who cannot tolerate enteral feeding or have gastrointestinal contraindications like bowel obstruction, fistulas, or severe ileus.
Research indicates that in severely malnourished patients or those with gastrointestinal malignancies, TPN can help restore nutritional deficits, support immune function, and enhance recovery, thereby reducing morbidity and mortality.
Adding specific nutrients such as glutamine and arginine has been associated with improved immune responses, shorter hospital stays, and fewer complications. Moreover, implementing perioperative nutritional strategies aligns with the principles of Enhanced Recovery After Surgery (ERAS), aiming to reduce metabolic stress and promote faster recovery.
Overall, individualized nutritional plans that include TPN when indicated play a crucial role in optimizing surgical outcomes. These strategies contribute to better wound healing, fewer infections, quicker mobilization, and an overall smoother postoperative course, especially in patients at high nutritional risk.
Key Takeaways on TPN in Surgical Recovery
Total Parenteral Nutrition (TPN) remains a crucial intervention for supporting postoperative recovery in patients unable to meet their nutritional needs enterally. Appropriate indication, timely initiation, meticulous management, and vigilant monitoring are essential to maximize benefits while minimizing risks. As part of a comprehensive, multidisciplinary approach, TPN helps improve wound healing, immune competence, and overall outcomes, ultimately contributing to reduced complications and enhanced recovery in vulnerable surgical populations. Upholding best practices and adhering to evidence-based guidelines will ensure optimal utilization of TPN, reinforcing its role as a lifesaving and recovery-supporting modality in modern surgical care.
References
- Total Parenteral Nutrition - StatPearls - NCBI Bookshelf
- Postoperative total parenteral nutrition - PubMed
- Postoperative parenteral nutrition in adults - UpToDate
- Perioperative Total Parenteral Nutrition in Surgical Patients
- When and how to start parenteral nutrition - Deranged Physiology
- Parenteral Nutrition: What it Is, Uses & Types - Cleveland Clinic
- 8.8 Total Parenteral Nutrition (TPN) – Clinical Procedures for Safer ...