TPN vs. Enteral Nutrition: What’s the Difference?
Understanding the Fundamentals of TPN and Enteral Nutrition
Nutritional support forms a cornerstone of medical care, especially for patients unable to meet their nutritional needs through regular oral intake. Among these, Total Parenteral Nutrition (TPN) and enteral nutrition are the primary modalities. Though both aim to deliver vital nutrients, they differ fundamentally in their routes, indications, benefits, and risks. This article explores these differences in depth, providing clarity on when and why each method is used, supported by current research and clinical guidelines.
Route of Administration and Physiological Impact
What are the main differences between total parenteral nutrition (TPN) and enteral nutrition?
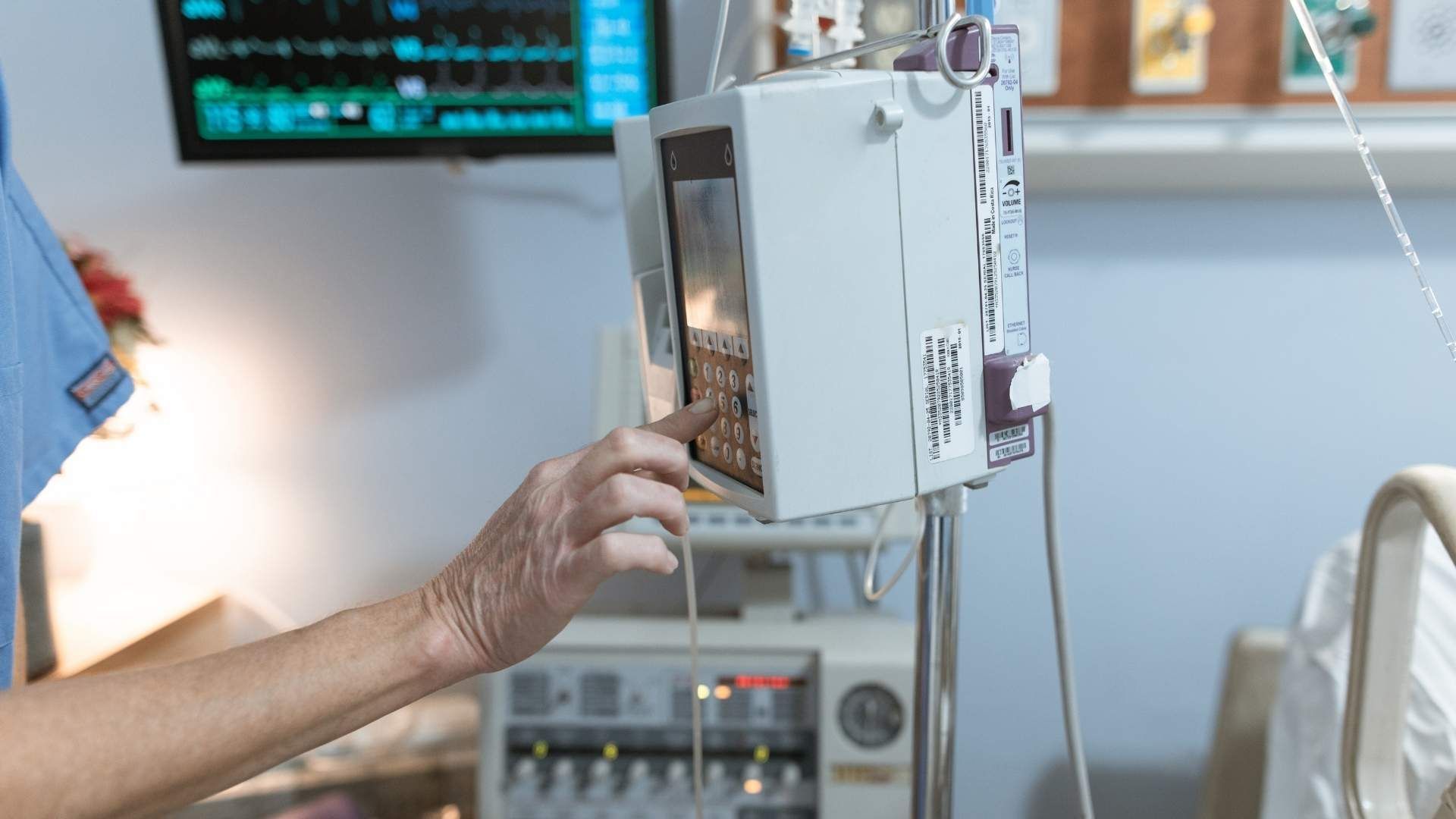
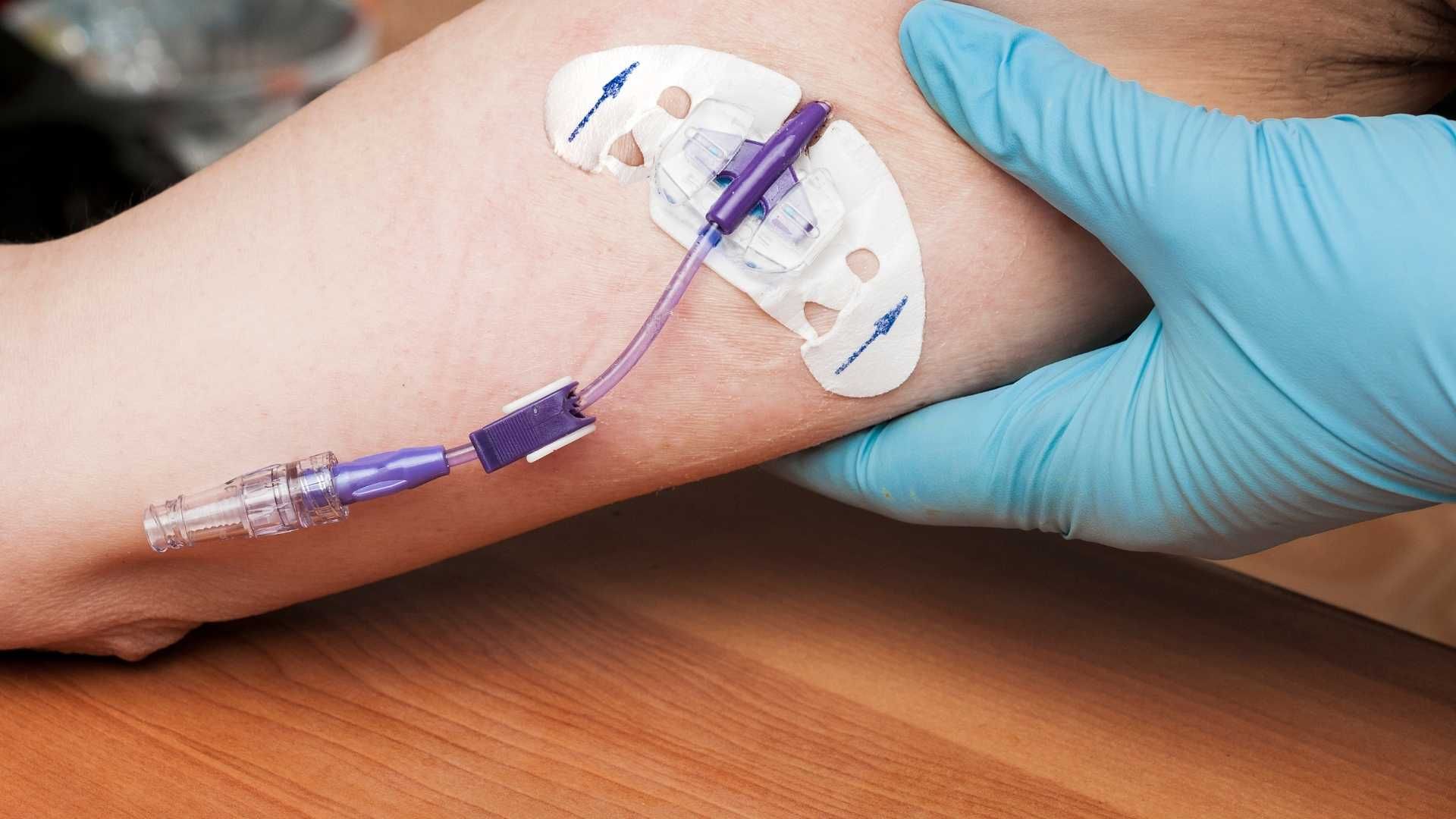
The most fundamental difference between TPN and enteral nutrition is the route through which nutrients are delivered to the patient. TPN involves delivering essential nutrients directly into the bloodstream via a central or peripheral vein using an intravenous catheter. This method bypasses the gastrointestinal tract entirely, making it suitable for patients whose digestive systems cannot be used. In contrast, enteral nutrition supplies nutrients through the gastrointestinal (GI) tract, either by mouth or through feeding tubes inserted into the nose, stomach, or small intestine, such as nasogastric or gastrostomy tubes.
Enteral nutrition is generally preferred when the gut is functional because it maintains gut integrity, stimulates normal digestive processes, and supports immune function. It is also usually simpler, safer, and less costly compared to TPN. TPN is reserved for situations where the GI tract cannot be used due to conditions like bowel obstruction, severe malabsorption, or extensive bowel resection. Both methods can deliver a variety of nutrients, including carbohydrates, amino acids, fats, vitamins, and electrolytes, but their management and complication profiles differ.
While TPN provides precise nutritional control, it carries higher risks such as bloodstream infections, blood clots, and metabolic disturbances. Enteral nutrition, on the other hand, can cause complications like aspiration pneumonia, diarrhea, or tube-related infections but typically involves fewer systemic risks.
Choosing between TPN and enteral nutrition depends on the patient’s clinical status, the functionality of the gut, and the urgency of nutritional requirements. Ideally, enteral feeding is initiated when feasible, with TPN used as a backup or when enteral nutrition is contraindicated.
Comparison of physiological effects of both methods
The physiological effects of these two nutritional delivery routes are markedly different, primarily in their interaction with the gut and systemic immune responses. Enteral nutrition actively engages the gastrointestinal system, maintaining mucosal integrity, promoting normal peristalsis, and supporting the gut-associated lymphoid tissue (GALT). This stimulation helps preserve gut barrier function and reduces bacterial translocation, lowering the risk of infections.
In contrast, TPN bypasses the gut, which can lead to decreased gut mucosal mass, increased intestinal permeability, and potential atrophy of intestinal tissues. This disuse may compromise immune responses and increase susceptibility to infections and systemic inflammation. Animal studies have demonstrated that enteral feeding is better at preserving immune function and reducing systemic inflammation compared to TPN.
This difference has important clinical implications. Patients receiving enteral nutrition tend to have fewer infectious complications and a shorter hospital stay, owing partly to the preservation of gut function. Conversely, TPN’s lack of gut stimulation may contribute to complications like bacterial overgrowth and translocation.
Impact on gut integrity and immune function
Maintaining gut integrity is crucial for overall health, especially in critically ill patients. Enteral nutrition helps sustain the structure and function of the gut mucosa by providing direct nutrients and mechanical stimulation. This reinforcement of the gut barrier prevents pathogenic bacteria from crossing into the bloodstream and supports the local immune system.
By preserving the gut’s integrity, enteral feeding reduces systemic inflammation and the risk of multi-organ failure. Additionally, gut-associated lymphoid tissue (GALT) plays a vital role in immune defense, which is stimulated and maintained through enteral nutrition.
On the other hand, TPN’s bypass of the GI tract deprives the gut of essential nutrients, leading to mucosal atrophy, decreased immune cell activity, and a higher risk of infections. The disuse of the gut can impair immune surveillance and facilitate bacterial translocation from the gut to systemic circulation.
In summary, the route of administration significantly influences physiological outcomes. Enteral nutrition supports the natural functions of the gastrointestinal tract and immune system, promoting better recovery and fewer complications. TPN, while lifesaving in specific cases, entails risks related to the absence of gut stimulation and increased likelihood of systemic infections.
| Aspect | Enteral Nutrition | Parenteral Nutrition | Additional Details |
|---|---|---|---|
| Route of administration | Via GI tract (mouth, feeding tubes) | Intravenous (vein access) | Central vs peripheral IV for TPN |
| Impact on gut | Preserves mucosal integrity, stimulates digestion | Leads to mucosal atrophy, gut disuse | Enteral supports gut immunity; TPN may weaken it |
| Immune function | Supports immune responses via gut-associated lymphoid tissue | May impair immune function due to disuse | Animal studies show better immune outcomes with EN |
| Risks and complications | Aspiration, diarrhea, tube site infection | Infection, bloodstream sepsis, thrombosis | Cost, management complexity, and complication profiles vary |
| Cost and management | Generally less expensive, easier to manage | More costly, requires sterile technique | Longer hospital stays may increase costs for TPN |
| Favorable conditions | Functional GI tract, no contraindications to feeding | Non-functional gut, contraindications to enteral | Choice depends on clinical assessment |
| Supporting evidence | Strong preference for enteral when possible | Used when enteral is contraindicated | Research continues to favor EN in many scenarios |
This comprehensive understanding underscores the importance of route selection in nutritional support, balancing physiological benefits with potential risks to optimize patient outcomes.
Clinical Indications and Patient Suitability
When should TPN be used instead of enteral nutrition?
Total parenteral nutrition (TPN) is essential when the gastrointestinal (GI) tract cannot be used or accessed safely. Conditions such as bowel obstruction, severe cases of bowel resection, high-output fistulas, or active GI bleeding make enteral feeding impossible or unsafe.
In situations where the GI tract is severely impaired, such as in extensive motility disorders or when there is a contraindication to the use of feeding tubes, TPN provides a direct route to deliver nutrients into the bloodstream. It is also indicated in hypercatabolic states like sepsis or trauma, where absorption is compromised.
Prolonged NPO (nothing by mouth) status exceeding one week, especially following major surgery or in critical illness, calls for TPN as a means to meet nutritional needs when enteral feeding is not feasible. Additionally, in cases of severe malabsorption or anatomical abnormalities preventing gut use, TPN becomes indispensable.
In summary, TPN is used over enteral nutrition when the gut cannot be used or when nutritional needs are not met through the GI tract, ensuring the patient receives necessary nutrients directly into the bloodstream, supporting recovery and sustaining life.
What clinical conditions favor the use of enteral nutrition?
Enteral nutrition is preferred for patients with a functioning GI tract who cannot consume food orally. This includes individuals with dysphagia due to stroke, neurological disorders, or facial trauma, where swallowing is impaired.
Patients recovering from gastrointestinal surgeries or suffering from gastrointestinal cancers often benefit from enteral feeding, as it helps maintain gut mucosal integrity and immune function. Conditions such as neuromuscular diseases, movement disorders, or critical injuries frequently require tube feeding to meet increased energy and protein requirements.
Enteral nutrition is also advantageous in cases where early initiation can reduce hospital stays and promote faster recovery. It supports the natural digestive processes, helps prevent mucosal atrophy, and lowers the risk of infections associated with invasive procedures like central line placements.
Overall, when the GI tract is functional but oral intake is contraindicated or insufficient, enteral nutrition becomes the first-line approach due to its physiological benefits and lower complication profile.
Assessment of GI tract functionality
The decision to use either TPN or enteral nutrition depends heavily on assessing the GI tract's functionality. Tests such as contrast studies, endoscopy, and clinical evaluation help determine if the gut can absorb and process nutrients.
If the GI tract demonstrates normal motility, absorption, and integrity, enteral nutrition is favored.
However, in cases with confirmed dysfunction, such as complete bowel obstruction, severe short bowel syndrome, or fistulas that prevent nutrient absorption, TPN is necessary.
Another consideration involves the patient's ability to tolerate feeding tubes, which depends on factors like risk of aspiration, presence of vomiting, or gastric emptying issues.
By accurately evaluating these factors, clinicians can choose the most appropriate route—enteral or parenteral—to optimize recovery and minimize complications.
Timing and duration of nutritional support
The timing and length of nutritional interventions are tailored to individual needs. Enteral nutrition is typically initiated early during hospitalization or recovery given its benefits in preserving gut function and immune response.
In acute settings, early initiation within 24-48 hours can improve outcomes, particularly if the patient has a functioning GI tract.
TPN may be reserved for cases where enteral feeding cannot be started promptly, or when it cannot be tolerated long-term due to ongoing contraindications.
The duration of TPN or enteral nutrition varies based on the clinical course. Short-term support spans days to weeks, such as post-surgical recovery, while long-term or indefinite support is used in chronic conditions like Crohn's disease or severe short bowel syndrome.
Monitoring and regular reassessment are critical to determine when to wean or adjust nutritional strategies, ensuring that support aligns with disease progression and recovery goals.
Risks and Complications

What are the key clinical considerations and risks associated with TPN and enteral nutrition?
Managing nutritional support in critically ill or hospitalized patients involves assessing numerous factors, including the functionality of the gastrointestinal (GI) tract, individual nutritional requirements, and specific contraindications. Enteral nutrition (EN) is usually preferred when the gut is working properly because it closely mimics natural digestion and supports immune function. It involves delivering nutrients via tubes inserted through the nose, mouth, or surgically into the stomach or small intestine.
Total parenteral nutrition (TPN), on the other hand, is reserved for situations where the GI tract cannot be used effectively, such as bowel obstructions, severe GI dysfunction, or post-gastrointestinal surgery. TPN delivers nutrients directly into the bloodstream via central or peripheral veins using specialized IV lines.
However, both methods carry specific risks. Enteral nutrition can lead to complications like aspiration pneumonia, diarrhea, constipation, dehydration, and infection at the insertion site of the feeding tube. These risks increase when feeding is not carefully monitored or when improper tube placement occurs.
TPN has its own set of challenges, including bloodstream infections related to catheter contamination, metabolic disturbances such as electrolyte imbalance or hyperglycemia, and liver issues like cholestasis with prolonged use. The insertion of central venous catheters poses risks such as vascular injury, thrombosis, or pneumothorax.
Monitoring patients on both types of nutrition involves regular checks of electrolytes, blood glucose, liver enzymes, triglyceride levels, and signs of infection. Proper management requires a multidisciplinary team including physicians, dietitians, and nursing staff, emphasizing early recognition of complications to mitigate adverse outcomes.
What are the benefits of enteral nutrition compared to TPN?
The advantages of enteral nutrition over TPN are well-documented in clinical research. EN helps preserve the physical integrity and function of the gut mucosa, which in turn maintains the barrier against bacteria and pathogens, reducing infection risk.
Supporting immune function is another critical benefit. Animal studies have shown that food in the gut plays an important role in systemic inflammation control and immune system regulation. EN encourages the release of gut hormones and maintains gut-associated lymphoid tissue, essential for immune defense.
Systematic reviews and multiple meta-analyses have demonstrated that EN is associated with lower mortality rates, fewer infections—particularly pneumonia and sepsis—and shorter hospital stays compared to TPN, especially in critically ill adults and postoperative patients.
Cost-effectiveness is also notable. EN is generally less expensive, easier to administer, and involves fewer invasive procedures, diminishing the likelihood of catheter-related infections and metabolic complications. It also promotes earlier initiation of feeding, which can facilitate recovery and reduce overall healthcare costs.
Another significant benefit is its physiological nature. EN stimulates the natural process of digestion and absorption, supports gut motility, and helps maintain normal blood flow to the GI tract. In contrast, TPN bypasses the gut entirely, which can lead to gut mucosal atrophy, bacterial overgrowth, and increased complications.
In summary, when the GI tract is functional, enteral nutrition offers numerous advantages, making it the preferred approach. It supports immune function, reduces infections and costs, and promotes better overall outcomes, thereby making it a critical component in nutritional management plans.
| Aspect | Enteral Nutrition | TPN | Additional Details |
|---|---|---|---|
| Route of Delivery | Via GI tract (tube or oral) | Intravenous | Bypasses the gut or uses it when functional |
| Risks | Aspiration, diarrhea, tube infection | Infection, metabolic disturbances, liver disease | Requires monitoring and skilled management |
| Cost | Generally less expensive | More costly | Cost varies with duration and complexity |
| Impact on Gut | Supports gut integrity and immune function | Can cause gut atrophy if used long-term | Importance of early EN when feasible |
| Infection Risk | Lower than TPN | Higher risk due to catheter | Vigilance needed in both methods |
| Suitability | When GI tract is functional | When GI is non-functional | Clinical decision based on patient status |
Overall, nutritional support strategies must be tailored carefully to each patient’s situation, with vigilant monitoring to minimize complications and maximize benefits.
Current Evidence and Research Findings

What are some recent research findings comparing TPN and enteral nutrition?
Over the past decade, numerous studies and reviews have focused on comparing total parenteral nutrition (TPN) and enteral nutrition (EN) to determine which method yields better patient outcomes.
Recent research overwhelmingly supports the use of enteral nutrition when the gastrointestinal (GI) tract is functional. Systematic reviews and meta-analyses published since 2008 have demonstrated that EN is associated with a lower risk of infections, including bloodstream infections and pneumonia, compared to TPN.
One of the most consistent findings is that EN reduces sepsis rates. For example, analyses show that patients receiving enteral feeding experience fewer infectious complications than those on TPN, with relative risks indicating a significant advantage for EN.
In terms of mortality, most studies reveal no clear difference between the two methods overall; however, some evidence suggests better survival rates in patients supported with EN, particularly in surgical and critically ill populations.
Hospital length of stay also tends to be shorter with EN. Patients using enteral feeding generally recover faster, experience fewer postoperative complications, and are discharged sooner than those requiring TPN.
This trend is especially evident in postoperative care for surgeries such as pancreaticoduodenectomy and gastrointestinal cancer resections, where enteral feeding supports gut integrity and immune function better than TPN.
Despite its benefits, TPN remains vital when the GI tract is completely non-functional or inaccessible. In such cases, TPN provides essential nutrients intravenously, ensuring survival when EN cannot be used.
Funding and cost considerations also favor EN, as it is less expensive and easier to manage, reducing overall healthcare costs.
Outcomes such as infection rates, mortality, hospital stay
| Outcome | EN Advantage | TPN Advantage | Additional Details |
|---|---|---|---|
| Infection risk | Lower | Higher | Entry and bloodstream infections are less common with EN |
| Mortality | Similar or Better | Slightly worse | Most studies show no significant difference, but some favor EN |
| Hospital length of stay | Shorter | Longer | Faster recovery and fewer complications with EN |
| Postoperative complications | Fewer | More | EN promotes gut health, reducing postoperative infections |
| Cost | Lower | Higher | EN is less costly, both in initial setup and ongoing management |
| Immune function | Preserved | Less preserved | Animal studies highlight that gut activity helps immune responses |
What are the recent research trends?
The current research landscape continues to endorse early and functional use of enteral nutrition for eligible patients. Emerging studies are exploring optimal timing, formulations, and delivery methods to maximize benefits.
Attention is also given to understanding the circumstances under which TPN may be preferable. These include cases with bowel obstruction, very short bowel syndrome, or severe GI injuries where early EN is contraindicated.
Moreover, research into the safety and complications of both methods emphasizes that while TPN carries higher risks of infections and metabolic disturbances, advances in catheter care, infection control, and monitoring have improved its safety profile.
Recent interest is also focused on home-based nutritional support, with studies examining the safety, quality of life, and health outcomes of long-term TPN and EN at home.
In summary, the overall research trend favors enteral nutrition for its physiological advantages, cost-effectiveness, and lower complication profile. TPN remains crucial for specific clinical situations but is increasingly viewed as a supportive or rescue intervention rather than the first-line option.
Summary and Future Perspectives
What are the main differences between TPN and enteral nutrition?
The main differences between total parenteral nutrition (TPN) and enteral nutrition lie in their routes of administration. TPN delivers nutrients directly into the bloodstream via intravenous access, effectively bypassing the gastrointestinal (GI) tract. In contrast, enteral nutrition supplies nutrients through the digestive system, either via oral intake or feeding tubes inserted into the nose, mouth, stomach, or small intestine.
Enteral nutrition is generally preferred when the GI tract remains functional because it preserves gut integrity, supports immune function, and is associated with fewer complications. It is also more straightforward, less costly, and safer compared to TPN.
TPN becomes necessary when the GI tract cannot be used due to obstructions, severe GI failure, or surgical removal of parts of the digestive system. Since it involves inserting a catheter into a large vein, usually near the heart, TPN carries risks such as bloodstream infections, blood clots, and metabolic disturbances like electrolyte imbalances.
The decision on which method to use depends heavily on the patient’s condition. When feasible, enteral nutrition is favored. However, TPN remains a critical intervention for individuals with non-functioning or inaccessible gut. Both approaches require a multidisciplinary team for proper management, careful monitoring, and adjustment based on nutritional needs and potential complications.
Emerging research and innovations
Recent advancements are focusing on improving the safety, efficacy, and sustainability of nutritional support. Innovations include the development of more sophisticated and individualized formulae tailored to specific patient needs, leveraging biotechnology for better nutrient stability, and minimizing adverse effects.
Research is also exploring the integration of sensors and digital health tools into infusion systems to monitor real-time biomarkers such as glucose, electrolytes, and hydration status. These technologies aim to prevent complications like hyperglycemia and electrolyte imbalances, especially in critically ill patients.
Emerging studies highlight the potential of microbiome-focused therapies, recognizing the importance of gut bacteria in immune response and disease management. Enhancing gut health through targeted probiotics or prebiotics in enteral nutrition could improve clinical outcomes.
Advances in catheter materials and insertion techniques are designed to reduce infection risks associated with TPN. Similarly, innovations in enteral feeding devices aim to decrease discomfort and improve patient adherence.
In addition, research into minimally invasive surgical procedures for long-term enteral access, such as advanced gastrostomy or jejunostomy techniques, promises to make nutritional support safer and more comfortable.
Guidelines for clinical practice
Current guidelines emphasize the importance of individualized nutritional assessment to determine the most appropriate route and method of delivery. The decision should consider the patient’s metabolic state, GI function, risk factors, and preferences.
For patients with a functional GI tract, early initiation of enteral nutrition is recommended, ideally within 24-48 hours of hospital admission for critically ill individuals, as evidenced by multiple clinical trials and meta-analyses.
In cases where enteral feeding is contraindicated or not tolerated, TPN should be employed cautiously, with vigilant monitoring for complications. The protocol involves regular assessment of blood glucose, electrolyte levels, liver function, and infection markers.
Both approaches should include strategies for preventing common complications. For example, preventing aspiration in enteral feeding involves elevating the head of the bed, while maintaining sterile technique and proper catheter care are vital in TPN.
Nutritional formulations should be customized, with adjustments based on ongoing monitoring, disease progression, and metabolic responses. Combining nutrition support with physiotherapy and other supportive care maximizes recovery.
The future of clinical practice in nutritional support is moving toward more precise, patient-centered approaches, integrating technological innovation, and evidence-based protocols to optimize outcomes and minimize risks.
| Aspect | TPN | Enteral Nutrition | Additional Details |
|---|---|---|---|
| Route of Delivery | Intravenous, into large veins | Via GI tract, through oral intake or tubes | Both require careful catheter or tube care |
| Use When | GI tract non-functional or inaccessible | GI tract functional, patient can swallow | Choice based on clinical condition |
| Benefits | Can be used in severe GI disease, long-term support | Preserves gut function, reduces infection risk | Cost-effective, easier management |
| Risks | Infection, blood clots, metabolic issues | Aspiration, diarrhea, tube site infections | Both need careful monitoring |
| Innovations | Sensor tech, microbiome therapies | Improved feeding devices, personalized formulas | Ongoing research into safety improvements |
Concluding Insights and Clinical Recommendations
Understanding the fundamental differences, indications, benefits, and risks of TPN and enteral nutrition helps clinicians make informed decisions tailored to individual patient needs. When the gastrointestinal tract is functional, enteral nutrition is usually the preferred choice due to its physiologic benefits, lower complication rates, and cost-effectiveness. TPN remains an essential modality for cases where the gut cannot be used, but it necessitates stringent monitoring and management to mitigate risks. Emerging research continues to reinforce the importance of early enteral feeding to improve outcomes, particularly in critically ill and surgical populations. Ultimately, personalized care, guided by clinical guidelines and evidence, ensures optimal nutritional support and patient recovery.
References
- Enteral vs. Parenteral Nutrition: A Complete Guide
- Enteral and Parenteral Nutrition
- Enteral vs. Parenteral Feeding & Nutrition: A Complete Guide
- Enteral and Parenteral Nutrition - BAPEN
- Advantages of enteral nutrition over parenteral nutrition - PMC
- Enteral versus parenteral nutrition and enteral versus a combination ...
- TPN vs. Tube Feeding: How Are They Different?
- Review Enteral vs total parenteral nutrition following major upper ...
- What is Parenteral Nutrition? - ASPEN