Understanding the Role of Carnitine in TPN and IDPN Therapy
Unlocking the Potential of Carnitine in Clinical Nutrition
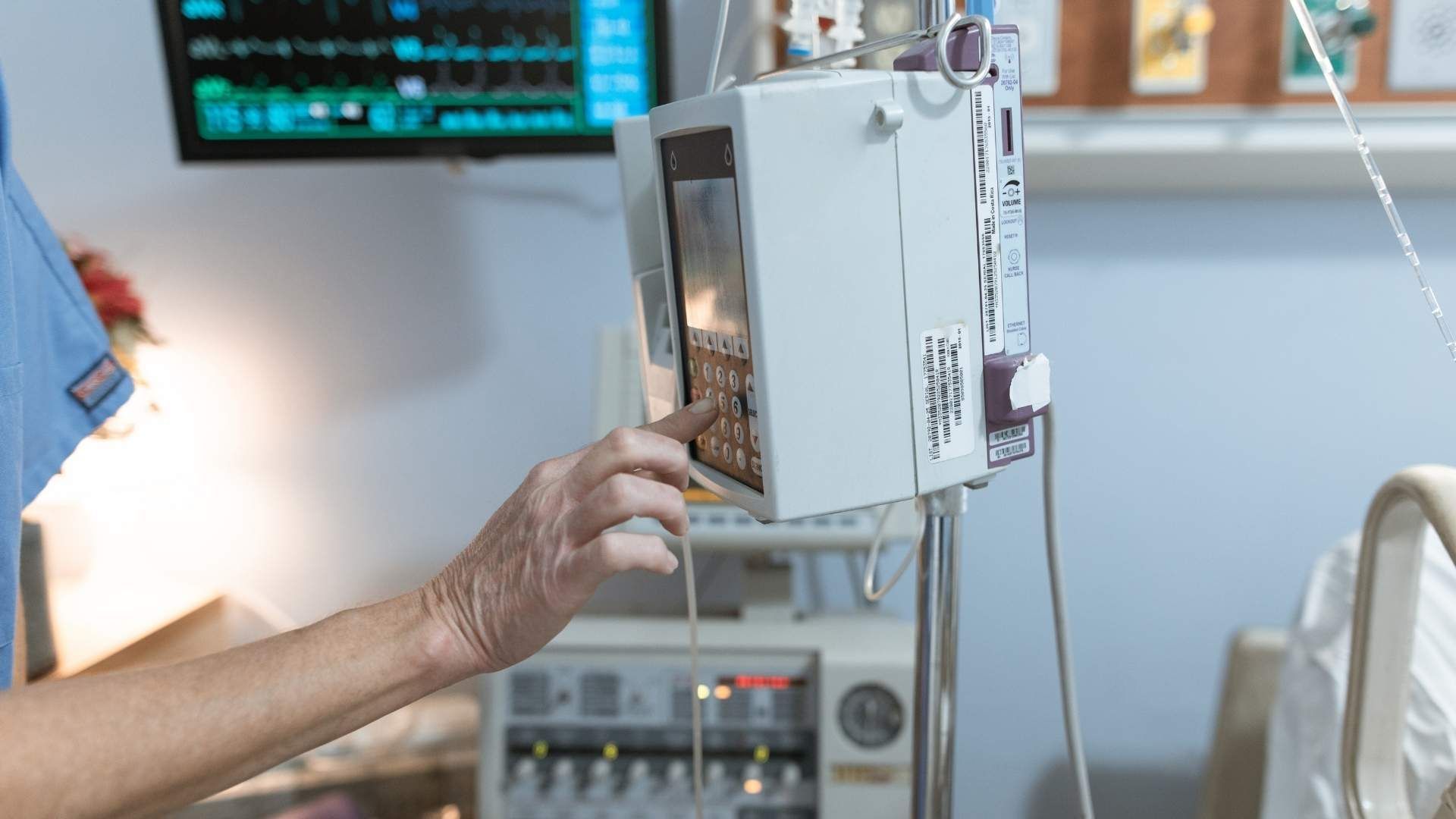
Carnitine plays a vital role in cellular energy metabolism, especially within the context of total parenteral nutrition (TPN) and intradialytic parenteral nutrition (IDPN). As a nutrient that facilitates fatty acid oxidation and mitochondrial energy production, its adequate presence is crucial for maintaining metabolic balance in vulnerable patient groups receiving artificial nutrition support. This article explores the mechanisms, clinical benefits, safety considerations, and current evidence underpinning the use of carnitine in TPN and IDPN, emphasizing its significance in improving patient outcomes across diverse medical settings.
Understanding Carnitine’s Role in Cellular Energy Metabolism
What is the role of carnitine in energy metabolism and cellular function?
Carnitine is a vital molecule that supports the body's cellular energy needs by facilitating the transport of long-chain fatty acids into mitochondria, the cell's energy powerhouses. Once inside the mitochondria, these fatty acids undergo β-oxidation, a process that generates ATP, the main energy currency of cells. This function is especially critical in tissues with high energy demands such as the heart and skeletal muscles.
Carnitine is produced naturally in the body from amino acids like lysine and methionine but can also be obtained through diet, mainly from animal products. Individuals on plant-based diets may have higher bioavailability of carnitine. It not only enables efficient fat utilization but also plays a role in carbohydrate metabolism and insulin sensitivity.
In cases of deficiency—whether primary due to genetic mutations affecting synthesis or secondary resulting from conditions like chronic illness or malnutrition—fatty acid oxidation becomes impaired. This can lead to clinical problems such as hypoglycemia, muscle weakness, and cardiomyopathy.
Research indicates that supplementing with carnitine can offer therapeutic benefits, particularly in health scenarios involving mitochondrial dysfunction. It helps restore energy production, reduce oxidative stress, and improve tissue function. For example, in patients receiving total parenteral nutrition (TPN) or intradialytic parenteral nutrition (IDPN), carnitine supplementation has been considered to support lipid metabolism and mitochondrial health.
Furthermore, studies have shown that intravenous carnitine administration effectively raises plasma carnitine levels quickly, which may be especially beneficial postoperatively or during critical illness. This boost can aid in reducing inflammation markers and potentially improve recovery outcomes.
Although clinical benefits such as improved lipid profiles, weight gain, or hospital stay reduction are not yet definitively established, current evidence underscores carnitine’s importance. It appears to help maintain muscle glycogen, support mitochondrial energy production, and possibly modulate inflammatory responses.
In summary, carnitine is essential for cellular energy metabolism, primarily by enabling fatty acid oxidation. Its supplementation, especially in clinical settings like TPN and IDPN, holds potential to support mitochondrial function, improve metabolic stability, and enhance recovery in various health conditions.
Why Carnitine is Added to TPN: Clinical Rationale and Benefits
Why is levocarnitine added to total parenteral nutrition (TPN)?
Several studies suggest that supplementing TPN with L-carnitine can improve fatty acid oxidation after a fat challenge and may also enhance nitrogen balance. Although these benefits are promising, further research is needed to confirm the consistency and significance of these effects.
Role in supporting fatty acid oxidation during TPN
L-carnitine acts as a vital shuttle, transporting long-chain fatty acids into mitochondria, where they are used for energy production. In TPN, especially for vulnerable patients such as preterm infants or critically ill individuals, carnitine ensures efficient utilization of lipids, preventing fat accumulation and promoting energy efficiency.
Prevention of metabolic disturbances related to lipid utilization
Patients receiving TPN or IDPN often face challenges in lipid processing, which can lead to metabolic issues like hyperlipidemia or energy deficits. Carnitine supplementation helps maintain proper fat oxidation, reducing the risk of metabolic disturbances and supporting overall nutritional status.
Impact on nitrogen balance and muscle preservation
Evidence indicates that L-carnitine may support nitrogen balance, helping preserve muscle mass in malnourished or catabolic states. Some studies also observed increased serum carnitine levels and reduced inflammatory markers following supplementation, which could contribute to better recovery and muscle tissue integrity.
| Aspect | Effect/Outcome | Additional Notes |
|---|---|---|
| Fatty acid oxidation | Improved post-fat challenge | Supports mitochondrial fatty acid entry |
| Lipid utilization | Better processing, fewer metabolic issues | Reduces fat buildup and related complications |
| Nitrogen balance | Potentially improved, aiding muscle preservation | Conflicting evidence suggests need for further research |
| Inflammatory response | Possible reduction with supplementation | May have anti-inflammatory effects |
While the evidence underscores the safety of carnitine supplementation in clinical settings, benefits such as improved lipid metabolism and muscle preservation warrant further investigation to establish routine use in TPN protocols.
Search query for further research: Carnitine supplementation in TPN clinical practice
Clinical Indications and Benefits of Carnitine Supplementation in Parenteral Nutrition
What are the indications and benefits of carnitine supplementation during parenteral nutrition?
Carnitine plays a crucial role as a shuttle for long-chain fatty acids, facilitating their entry into mitochondria for energy production. Its importance becomes especially apparent in patients receiving total parenteral nutrition (PN), such as preterm infants or critically ill individuals, who are at risk of developing carnitine deficiency due to lower reserves and lack of dietary intake.
In such scenarios, supplementing with L-carnitine can increase plasma carnitine levels, aiding in fat oxidation and energy metabolism. This is particularly relevant during episodes of trauma or surgeries like esophagectomy, where there may be a reduction in the total body carnitine pool, impairing lipid utilization.
While plasma levels of carnitine often rise with supplementation, the clinical benefits—such as improved lipid profiles, weight gain, or reduced hospital stay—are not consistently demonstrated across studies. In some cases, carnitine infusion has been used to correct deficiencies, particularly when levels are low, and has been associated with better management of cholestasis related to parenteral nutrition.
Supplementation doses typically range from 2-5 mg per kg per day for nutritional support, with pharmacological doses of 50-100 mg per kg per day used for detoxification or specific deficiencies. Monitoring involves measuring blood and urine levels to assess deficiency and guide therapy.
Importantly, even if plasma levels increase, the evidence for broad, additional metabolic benefits in all patient groups is limited. Therefore, routine prophylactic use in PN, especially in preterm infants, remains controversial unless deficiency is confirmed.
How safe is carnitine supplementation?
Overall, L-carnitine supplementation during PN has been found to be well tolerated. Adverse events are mostly mild or moderate, and serious side effects are rare or absent. Studies involving critically ill patients and postoperative individuals show that intravenous administration is safe over short durations, such as 3-4 days.
Some studies also observed an anti-inflammatory effect indicated by a greater reduction in C-reactive protein (CRP) levels postoperatively when carnitine was added to PN, suggesting a potential benefit beyond metabolic support.
Urinary carnitine excretion can increase significantly with supplementation; however, this does not typically result in toxicity. Muscle carnitine levels tend to remain unchanged, and lipid and energy metabolism parameters are generally unaffected in the short term.
In conclusion, intravenous carnitine supplementation during parenteral nutrition appears safe and may be beneficial in correcting deficiencies, supporting lipid metabolism, and possibly reducing inflammation in specific patient populations. Nonetheless, routine prophylactic use in all patients is not currently supported by definitive evidence.
Safety, Efficacy, and Regulatory Aspects of Carnitine Supplementation
What is known about the safety and regulatory aspects of carnitine supplementation in TPN and IDPN therapies?
Carnitine supplementation in total parenteral nutrition (TPN) and intradialytic parenteral nutrition (IDPN) is generally regarded as safe when administered within recommended doses and under proper clinical supervision. It is especially useful in specific patient groups, such as preterm infants on TPN, who are at risk of deficiency due to lower reserves and limited dietary intake.
In critically ill patients receiving TPN, intravenous L-carnitine has been shown to increase plasma carnitine levels effectively. While this boosts circulating levels, clinical benefits such as improved lipid utilization, energy metabolism, or nitrogen balance are not consistently demonstrated. Nonetheless, the supplementation is considered safe, with studies showing no significant adverse effects and most side effects being mild or moderate.
The doses commonly used in clinical practice often reach up to 50 mg/kg per day, administered intravenously over several days. In cases of carnitine deficiency, especially among patients with renal failure or those with cholestasis linked to long-term PN, supplementation is supported by regulatory guidelines and clinical evidence.
Regulatory authorities support carnitine use in particular scenarios, including the treatment of muscle weakness, anemia, and certain metabolic disturbances. Safety concerns primarily involve potential interactions with medications such as pivalate-containing antibiotics and anticonvulsants, which can lower endogenous carnitine levels or interfere with its metabolism.
Monitoring for adverse events is important, especially at higher doses (~3 grams/day), where side effects such as gastrointestinal discomfort, body odor, or rare allergic reactions may occur. Regular assessment of levels and symptoms helps ensure safety during therapy.
Overall, the use of carnitine in parenteral nutrition settings aligns with strict medical guidelines, emphasizing individualized dosing and vigilant monitoring to maintain safety while maximizing potential benefits.
Clinical Evidence Supporting the Use of Carnitine in Nutritional Support
What evidence supports the beneficial effects of carnitine in patients receiving nutritional support?
Research indicates that carnitine is a vital molecule in lipid metabolism, especially in patients undergoing parenteral nutrition (PN) or intradialytic parenteral nutrition (IDPN). Carnitine functions as a shuttle, transporting long-chain fatty acids into mitochondria for β-oxidation, which is essential for energy production.
In various clinical settings such as dialysis, neonatal care, and critical illness, supplementing with L-carnitine has demonstrated increased plasma levels, confirming its bioavailability. For example, in patients receiving TPN, supplementation raises plasma total carnitine and free carnitine levels significantly. This increase suggests an improved capacity for fatty acid oxidation, potentially supporting energy needs.
Although increased plasma levels are a clear biochemical outcome, clinical benefits like improved lipid profiles, weight gain, or reduced hospital stay have been inconsistent across studies. Nonetheless, some evidence suggests that carnitine supplementation can help maintain muscle glycogen levels and reduce inflammatory markers such as C-reactive protein (CRP), which is particularly relevant in postoperative patients.
Furthermore, in patients on dialysis or with liver disorders, carnitine deficiencies are common due to lower reserves and lack of dietary intake. Supplementation in these groups has been associated with improved symptoms such as neuropathy and anemia, indicating a broader role in supporting metabolic functions and overall nutritional status.
In neonates and preterm infants receiving PN, prophylactic L-carnitine is considered to mitigate deficiency risks, though current evidence does not strongly support routine supplementation without deficiency. When deficiency is identified, intravenous infusion of carnitine at high doses has been successfully used to correct levels and potentially improve clinical outcomes.
Safety data from multiple studies confirm that intravenous administration of carnitine during PN is well-tolerated, with mostly mild adverse effects and no significant acute side effects noted.
In conclusion, while biochemical and metabolic markers improve with carnitine supplementation, the definitive clinical benefits, including enhanced growth, reduced complications, or faster recovery, are less consistent according to current evidence. Nevertheless, maintaining adequate carnitine levels appears crucial for optimal fatty acid metabolism and energy production in patients receiving TPN or IDPN.
Carnitine in special patient groups: Neonates and those with renal disease
What is known about the use of carnitine in neonatal and renal patient populations?
In preterm infants receiving total parenteral nutrition (PN), routine prophylactic supplementation of L-carnitine is generally not supported by clinical evidence. Although these infants are at increased risk of carnitine deficiency due to limited reserves and absence of dietary intake, studies have yet to demonstrate consistent improvements in clinical outcomes such as lipid profiles, weight gain, or reduced hospital stays following supplementation.
Despite this, ensuring adequate carnitine levels remains important because deficiency has been associated with cholestasis, which can cause serious liver complications. In cases where cholestasis is refractory or severe, measuring carnitine levels and considering intravenous carnitine infusions are recommended. Such treatment can help improve liver function and support lipid metabolism.
For patients with renal failure, especially those on hemodialysis, carnitine deficiency is a common concern. These patients often have lower stores of native carnitine and experience its depletion through dialysis processes. Supplementation with intravenous or intradialytic carnitine has been shown to boost plasma levels, potentially improving associated metabolic issues, such as muscle weakness, fatigue, and anemia.
Evidence suggests that intradialytic carnitine administration is largely safe and can moderate some metabolic disturbances related to deficiency. It also supports mitochondrial function and fat metabolism, which are crucial in maintaining energy levels in renal patients.
Overall, targeted management of carnitine deficiency—either through monitoring levels or considering replacement in high-risk groups—aims to improve metabolic stability, prevent deficiency-related complications like muscle wasting and liver dysfunction, and enhance overall patient health.
| Patient Group | Indications for Carnitine Use | Expected Benefits | Additional Notes |
|---|---|---|---|
| Preterm infants | Refractory cholestasis when deficiency suspected | Improved liver function, lipid metabolism | Not routinely recommended in prophylactic form |
| Hemodialysis patients | Depletion during dialysis | Increased plasma levels, reduced muscle weakness | Considered safe; supports energy production |
| Long-term PN patients | Risk of deficiency leading to cholestasis | Prevention of cholestasis, support of lipid utilization | Measurement recommended if cholestasis present |
This targeted application aligns with the understanding that carnitine is vital for fatty acid transport into mitochondria, acting as a shuttle for long-chain fatty acids to facilitate energy production.
Postoperative and Short-term Parenteral Post Care with Carnitine
What are the effects of intravenous carnitine during postoperative PN support?
Intravenous carnitine has shown promising effects when added to parenteral nutrition (PN) during the postoperative period. It significantly increases serum carnitine levels, which can be beneficial for patients undergoing surgery, especially those with pre-existing deficiencies or increased metabolic demands.
Research indicates that short-term administration, typically lasting 3 to 4 days, can lead to reductions in inflammatory markers like C-reactive protein (CRP). This suggests an anti-inflammatory role for carnitine, which may help mitigate systemic inflammation associated with surgical stress.
Furthermore, studies demonstrate that intravenous carnitine can support mitochondrial function by providing the necessary substrate for fatty acid oxidation. Although muscle ATP and phosphocreatine levels tend to remain unchanged, glycogen levels in muscle are maintained better with carnitine supplementation compared to non-supplemented controls.
Impact on inflammatory markers like CRP
A notable outcome observed with carnitine supplementation is the greater decrease in CRP levels postoperatively. This reduction in inflammation markers hints at potential benefits that include improved immune response and recovery process.
The anti-inflammatory effects appear to be linked with carnitine’s role in enhancing fat metabolism and energy production at the cellular level, which may attenuate the systemic inflammatory response triggered by surgery.
Safety considerations in acute postoperative scenarios
In the context of short-term use, intravenous carnitine has been found to be safe. Adverse events are mostly mild or moderate, with no significant acute side effects reported during infusions.
Routine monitoring of serum carnitine levels is recommended, especially in cases where deficiency is suspected or in patients with complex metabolic needs. The overall safety profile supports its use as an adjunct therapy during early postoperative recovery.
In summary, adding intravenous carnitine to PN in the postoperative setting offers a promising strategy to enhance recovery, reduce inflammation, and support mitochondrial function with minimal safety concerns when used appropriately.
Interaction of Lipid Emulsions and Carnitine in IDPN and TPN
How do lipid emulsions in IDPN interact with carnitine supplementation?
Lipid emulsions used in Intradialytic Parenteral Nutrition (IDPN) and Total Parenteral Nutrition (TPN) typically consist of soybean oil or mixed lipid formulations. These provide essential fatty acids and calories necessary for patients unable to maintain adequate nutrition through oral intake. The composition of these lipid emulsions influences how effectively lipids are metabolized and can impact inflammatory responses.
Carnitine plays a crucial role in lipid metabolism by acting as a shuttle for long-chain fatty acids. It transports fatty acids into mitochondria where β-oxidation occurs, facilitating energy production from fats. When lipid emulsions are infused intravenously, especially in critically ill or malnourished patients, efficient fatty acid oxidation is vital to prevent lipid accumulation and reduce inflammation.
Studies have shown that plasma triglyceride and free fatty acid levels tend to rise during fat infusion but typically normalize within 24 hours. This suggests a transient state of lipid metabolism that carnitine can help manage by improving the transport and utilization of fatty acids.
While clinical evidence has not consistently shown that carnitine supplementation significantly alters lipid parameters, its role in supporting fatty acid transport remains beneficial. By enhancing fatty acid oxidation, carnitine could potentially reduce the risk of lipid buildup, lower inflammation, and improve overall metabolic efficiency during TPN or IDPN.
Additionally, in scenarios where fat metabolism might be compromised—such as in critically ill or postoperative patients—carnitine supplementation might assist in optimizing lipid utilization, ultimately supporting better energy production and recovery.
In conclusion, the interaction of lipid emulsions with carnitine supplementation in TPN and IDPN involves improving lipid clearance and utilization, which could translate into minimized inflammatory responses and enhanced metabolic health. Nevertheless, more robust evidence is needed to firmly establish routine supplementation benefits, but current understanding underscores its potential importance in clinical nutrition management.
Monitoring and Assessment of Carnitine Status in Parenteral Nutrition
How should clinicians monitor carnitine levels during TPN/IDPN therapy?
Monitoring carnitine levels in patients receiving total parenteral nutrition (TPN) or intradialytic parenteral nutrition (IDPN) is essential to ensure optimal metabolic support and prevent deficiencies or toxicity.
Laboratory assessments typically involve measuring plasma and urinary carnitine concentrations. Blood tests can reveal low plasma free or total carnitine levels, which may indicate a deficiency—common in preterm infants or patients undergoing dialysis. Elevated urinary excretion of carnitine can also serve as an indicator of how much carnitine is being utilized or lost during therapy.
These measurements help clinicians determine whether a patient's carnitine stores are adequate or if supplementation adjustments are necessary. For example, increased urinary loss might suggest a need for higher doses, while very low plasma levels could warrant active infusions.
Regular monitoring should combine these lab results with clinical assessments. Signs like muscle weakness, fatigue, or abnormal metabolic profiles can further guide management. The goal is to maintain carnitine within a safe, effective range.
Adjustment of supplementation doses must be individualized. Doses should be increased cautiously if deficiency signs are evident, and decreased if levels are high or if there are signs of toxicity. Overall, ongoing evaluation ensures therapy remains beneficial and safe.
In summary, systematic blood and urine testing, combined with clinical evaluation, forms the basis of effective monitoring of carnitine status during TPN and IDPN therapy, optimizing patient outcomes and minimizing risks.
Summary and Future Directions in Carnitine Use in Parenteral Nutrition
What is the outlook for carnitine supplementation in TPN and IDPN based on current research?
Research indicates that carnitine plays a vital role in fat metabolism and mitochondrial energy production, which are crucial during parenteral nutrition (PN) and intradialytic parenteral nutrition (IDPN). Numerous studies show that intravenous administration of carnitine can effectively elevate plasma levels in critically ill or malnourished patients, including those undergoing hemodialysis or postoperative recovery.
In patients receiving total parenteral nutrition, especially preterm infants and those with liver or kidney disease, carnitine deficiency has been noted. Supplementation in such cases has been associated with higher plasma levels and some improvements in glycogen preservation and inflammatory markers like CRP. However, the clinical benefits—such as enhanced lipid utilization, weight gain, or reduced hospital stay—are not consistently demonstrated across different studies.
Safety profiles for intravenous carnitine are generally favorable, with mostly mild adverse events and no significant acute side effects reported. This suggests that supplementation is well tolerated in various patient populations.
Despite promising biochemical effects, current evidence does not support routine prophylactic use in all PN patients. Instead, targeted supplementation may be considered in cases of confirmed deficiency, especially when clinical signs of impaired fatty acid oxidation or cholestasis are present.
Ongoing research aims to clarify which specific groups will benefit the most from carnitine therapy and to optimize dosing regimens. Emerging personalized nutrition strategies, guided by biomarkers and individual metabolic profiles, hold promise for improving the efficacy and precision of carnitine use in clinical nutrition.
Overall, the outlook for carnitine in TPN and IDPN is optimistic, with future directions focusing on individualized approaches, better understanding of its mechanisms, and establishing clear guidelines on when and how to use supplementation for maximum benefit.
Enhancing Parenteral Nutrition with Carnitine: Clinical Insights and Outlook
Carnitine plays a pivotal role in the metabolic support provided by TPN and IDPN, chiefly by supporting fatty acid oxidation and mitochondrial energy production. Its supplementation benefits various patient populations, particularly those at risk of deficiency, such as preterm infants, dialysis patients, and individuals experiencing metabolic disturbances. Safety profiles are reassuring when used appropriately, and monitoring is critical for optimal management. Although evidence continues to evolve, the integration of carnitine into personalized nutritional strategies holds promise for improving clinical outcomes. Future research will likely clarify its full therapeutic potential, supporting more targeted and effective use in clinical nutrition support.
References
- Newsletters: Carnitine – Who Needs It? - Oley Foundation
- Intradialytic parenteral nutrition in maintenance hemodialysis ...
- Effects of L-carnitine supplemented total parenteral nutrition on lipid ...
- The effect of carnitine supplemented total parenteral nutrition on ...
- A systematic review about prophylactic L-carnitine administration in ...
- [PDF] Management of PN-induced Cholestasis
- [PDF] Intradialytic Parenteral Nutrition (IDPN) - BC Renal
- Intravenous Carnitine Administration in Addition to Parenteral ...
- [PDF] Pocket Guide to Nutrition Assessment of the Patient with Kidney ...